

Combining α-Radioimmunotherapy and Adoptive T Cell Therapy to Potentiate Tumor Destruction
- PMID: 26098691
- PMCID: PMC4476754
- DOI: 10.1371/journal.pone.0130249
Combining α-Radioimmunotherapy and Adoptive T Cell Therapy to Potentiate Tumor Destruction
Abstract
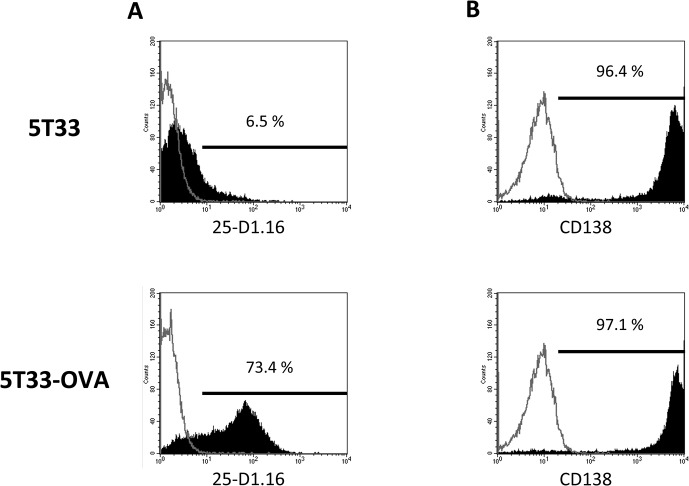
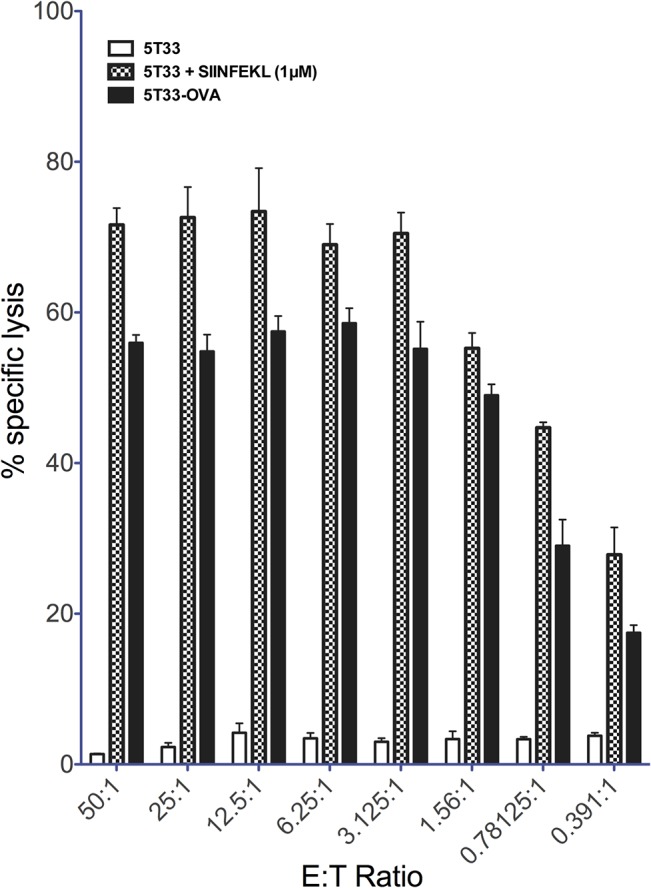
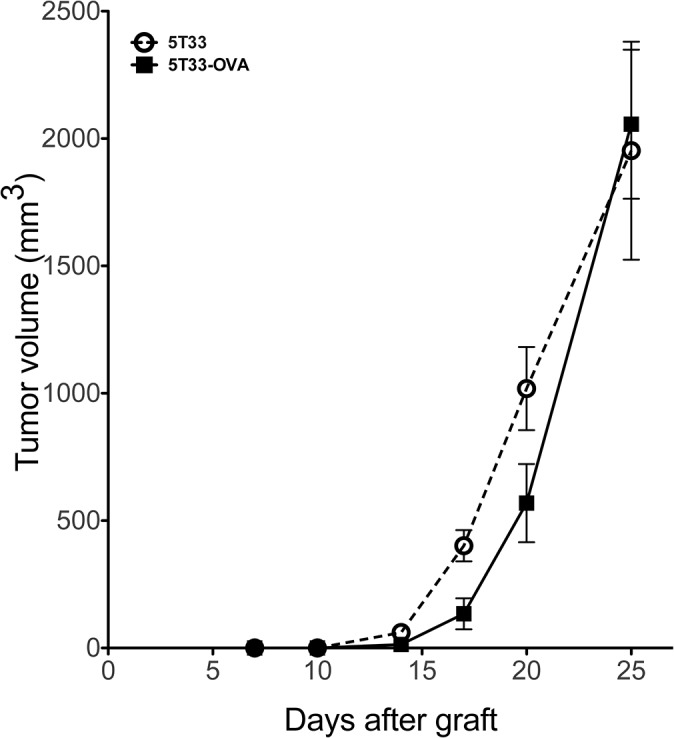
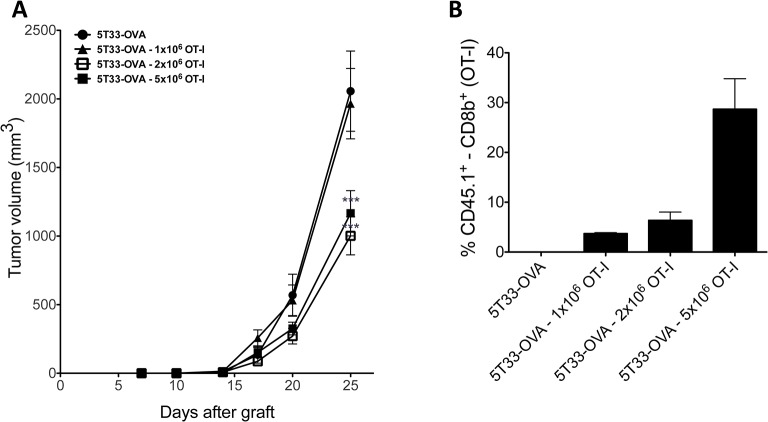
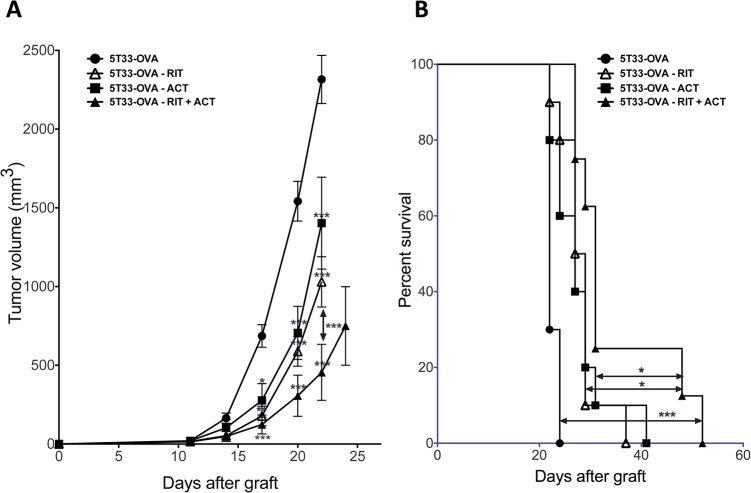
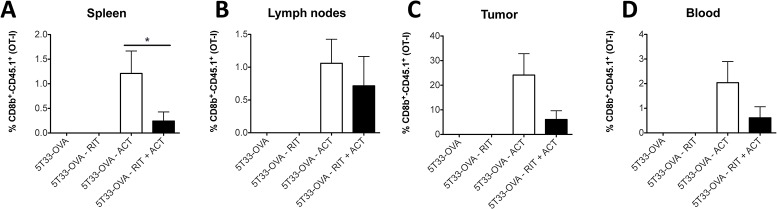
Ionizing radiation induces direct and indirect killing of cancer cells and for long has been considered as immunosuppressive. However, this concept has evolved over the past few years with the demonstration that irradiation can increase tumor immunogenicity and can actually favor the implementation of an immune response against tumor cells. Adoptive T-cell transfer (ACT) is also used to treat cancer and several studies have shown that the efficacy of this immunotherapy was enhanced when combined with radiation therapy. α-Radioimmunotherapy (α-RIT) is a type of internal radiotherapy which is currently under development to treat disseminated tumors. α-particles are indeed highly efficient to destroy small cluster of cancer cells with minimal impact on surrounding healthy tissues. We thus hypothesized that, in the setting of α-RIT, an immunotherapy like ACT, could benefit from the immune context induced by irradiation. Hence, we decided to further investigate the possibilities to promote an efficient and long-lasting anti-tumor response by combining α-RIT and ACT. To perform such study we set up a multiple myeloma murine model which express the tumor antigen CD138 and ovalbumine (OVA). Then we evaluated the therapeutic efficacy in the mice treated with α-RIT, using an anti-CD138 antibody coupled to bismuth-213, followed by an adoptive transfer of OVA-specific CD8+ T cells (OT-I CD8+ T cells). We observed a significant tumor growth control and an improved survival in the animals treated with the combined treatment. These results demonstrate the efficacy of combining α-RIT and ACT in the MM model we established.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
