

Antibiotics for acute otitis media in children
- PMID: 26099233
- PMCID: PMC7043305
- DOI: 10.1002/14651858.CD000219.pub4
Antibiotics for acute otitis media in children
Update in
-
Antibiotics for acute otitis media in children.Cochrane Database Syst Rev. 2023 Nov 15;11(11):CD000219. doi: 10.1002/14651858.CD000219.pub5. Cochrane Database Syst Rev. 2023. PMID: 37965923 Free PMC article.
Abstract
Background: Acute otitis media (AOM) is one of the most common diseases in early infancy and childhood. Antibiotic use for AOM varies from 56% in the Netherlands to 95% in the USA, Canada and Australia. This is an update of a Cochrane review first published in The Cochrane Library in Issue 1, 1997 and previously updated in 1999, 2005, 2009 and 2013.
Objectives: To assess the effects of antibiotics for children with AOM.
Search methods: We searched CENTRAL (2015, Issue 3), MEDLINE (1966 to April week 3, 2015), OLDMEDLINE (1958 to 1965), EMBASE (January 1990 to April 2015), Current Contents (1966 to April 2015), CINAHL (2008 to April 2015) and LILACS (2008 to April 2015).
Selection criteria: Randomised controlled trials (RCTs) comparing 1) antimicrobial drugs with placebo and 2) immediate antibiotic treatment with expectant observation (including delayed antibiotic prescribing) in children with AOM.
Data collection and analysis: Two review authors independently assessed trial quality and extracted data.
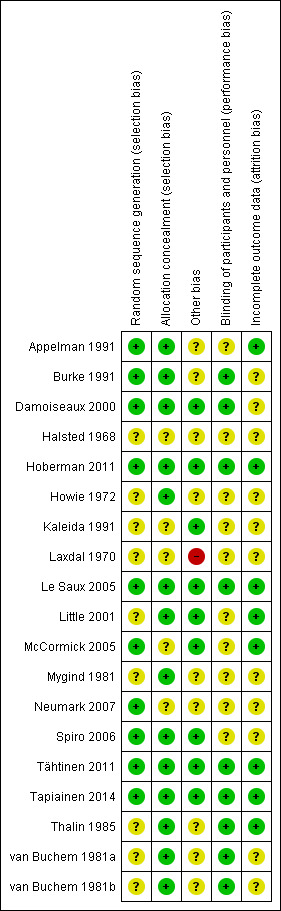
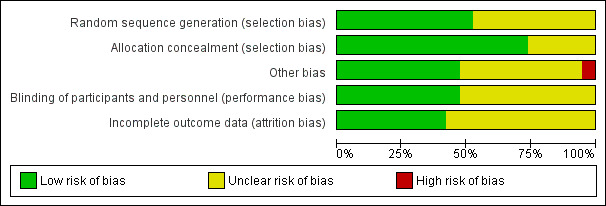
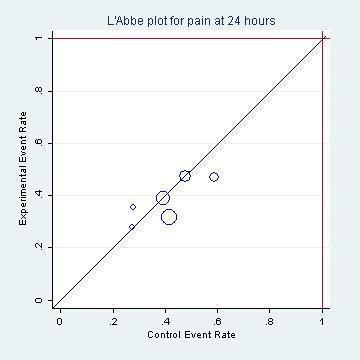
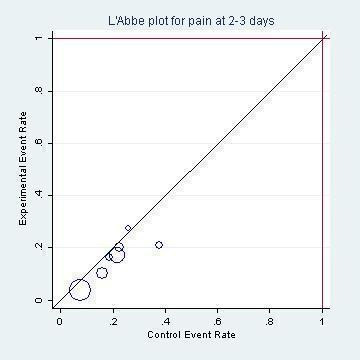
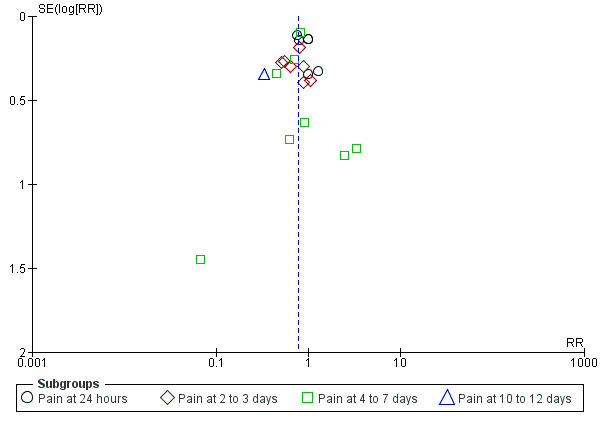
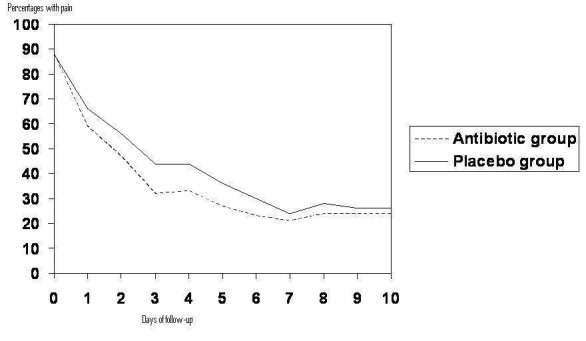
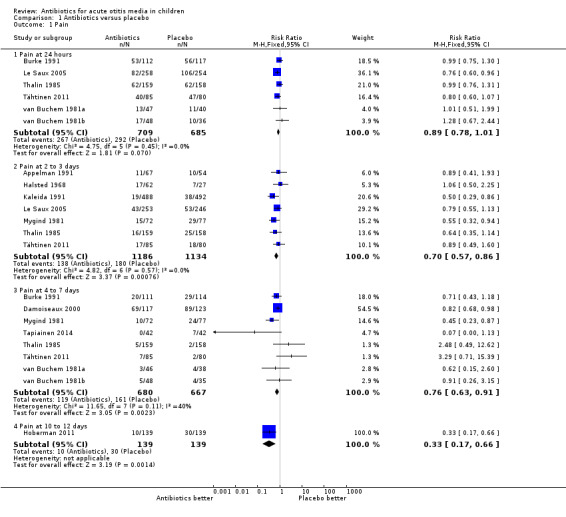
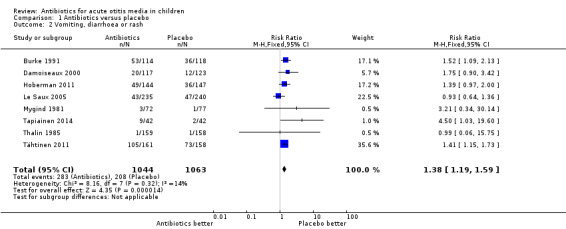
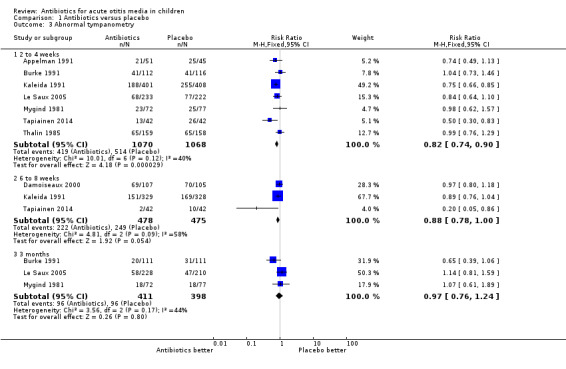
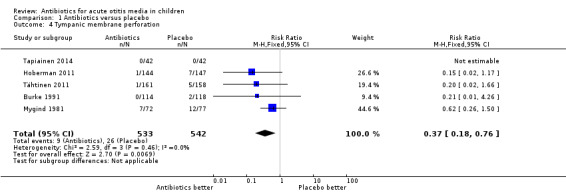
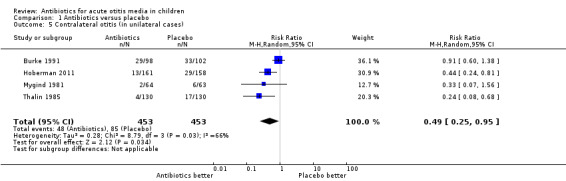
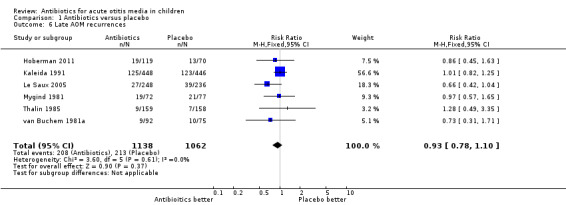
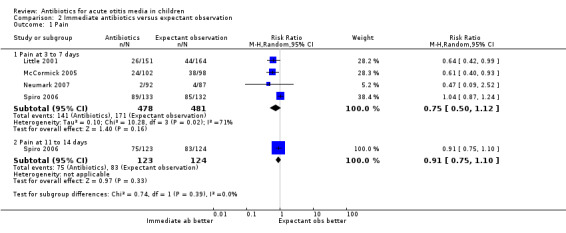
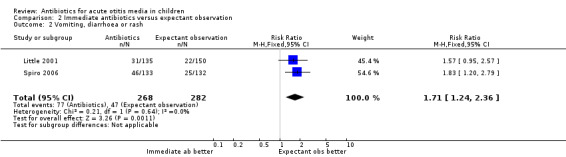
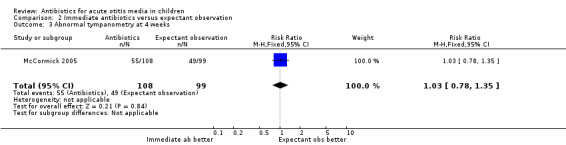
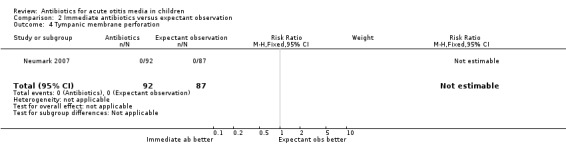
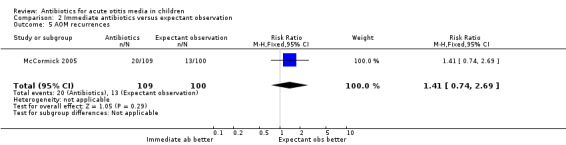
Main results: For the review of antibiotics against placebo, 13 RCTs (3401 children and 3938 AOM episodes) from high-income countries were eligible and had generally low risk of bias. The combined results of the trials revealed that by 24 hours from the start of treatment, 60% of the children had recovered whether or not they had placebo or antibiotics. Pain was not reduced by antibiotics at 24 hours (risk ratio (RR) 0.89, 95% confidence interval (CI) 0.78 to 1.01) but almost a third fewer had residual pain at two to three days (RR 0.70, 95% CI 0.57 to 0.86; number needed to treat for an additional beneficial outcome (NNTB) 20). A quarter fewer had pain at four to seven days (RR 0.76, 95% CI 0.63 to 0.91; NNTB 16) and two-thirds fewer had pain at 10 to 12 days (RR 0.33, 95% CI 0.17 to 0.66; NNTB 7) compared with placebo. Antibiotics did reduce the number of children with abnormal tympanometry findings at two to four weeks (RR 0.82, 95% CI 0.74 to 0.90; NNTB 11), at six to eight weeks (RR 0.88, 95% CI 0.78 to 1.00; NNTB 16) and the number of children with tympanic membrane perforations (RR 0.37, 95% CI 0.18 to 0.76; NNTB 33) and halved contralateral otitis episodes (RR 0.49, 95% CI 0.25 to 0.95; NNTB 11) compared with placebo. However, antibiotics neither reduced the number of children with abnormal tympanometry findings at three months (RR 0.97, 95% CI 0.76 to 1.24) nor the number of children with late AOM recurrences (RR 0.93, 95% CI 0.78 to 1.10) when compared with placebo. Severe complications were rare and did not differ between children treated with antibiotics and those treated with placebo. Adverse events (such as vomiting, diarrhoea or rash) occurred more often in children taking antibiotics (RR 1.38, 95% CI 1.19 to 1.59; number needed to treat for an additional harmful outcome (NNTH) 14). Funnel plots do not suggest publication bias. Individual patient data meta-analysis of a subset of included trials found antibiotics to be most beneficial in children aged less than two years with bilateral AOM, or with both AOM and otorrhoea.For the review of immediate antibiotics against expectant observation, five trials (1149 children) from high-income countries were eligible and had low to moderate risk of bias. Four trials (1007 children) reported outcome data that could be used for this review. From these trials, data from 959 children could be extracted for the meta-analysis of pain at three to seven days. No difference in pain was detectable at three to seven days (RR 0.75, 95% CI 0.50 to 1.12). One trial (247 children) reported data on pain at 11 to 14 days. Immediate antibiotics were not associated with a reduction in the number of children with pain (RR 0.91, 95% CI 0.75 to 1.10) compared with expectant observation. Additionally, no differences in the number of children with abnormal tympanometry findings at four weeks, tympanic membrane perforations and AOM recurrence were observed between groups. No serious complications occurred in either the antibiotic or the expectant observation group. Immediate antibiotics were associated with a substantial increased risk of vomiting, diarrhoea or rash compared with expectant observation (RR 1.71, 95% CI 1.24 to 2.36; NNTH 9).Results from an individual patient data meta-analysis including data from six high-quality trials (1643 children) that were also included as individual trials in our review showed that antibiotics seem to be most beneficial in children younger than two years of age with bilateral AOM (NNTB 4) and in children with both AOM and otorrhoea (NNTB 3).
Authors' conclusions: This review reveals that antibiotics have no early effect on pain, a slight effect on pain in the days following and only a modest effect on the number of children with tympanic perforations, contralateral otitis episodes and abnormal tympanometry findings at two to four weeks and at six to eight weeks compared with placebo in children with AOM. In high-income countries, most cases of AOM spontaneously remit without complications. The benefits of antibiotics must be weighed against the possible harms: for every 14 children treated with antibiotics one child experienced an adverse event (such as vomiting, diarrhoea or rash) that would not have occurred if antibiotics were withheld. Therefore clinical management should emphasise advice about adequate analgesia and the limited role for antibiotics. Antibiotics are most useful in children under two years of age with bilateral AOM, or with both AOM and otorrhoea. For most other children with mild disease in high-income countries, an expectant observational approach seems justified.
Conflict of interest statement
Chris Del Mar (CDM) declares no conflicts of interests in the current work. Maroeska M. Rovers (MMR) has participated in workshops and educational activities on otitis media organised by GlaxoSmithKline and received a grant from GlaxoSmithKline for a study on the microbiology of otitis media in 2009. Roderick P. Venekamp (RPV) is an Editor of the Cochrane Acute Respiratory Infections Group. Sharon L Sanders (SLS) declares no conflicts of interests in the current work. Paul P Glasziou (PPG) is co‐investigator on NHMRC funded grant Antibiotic Resistance.
Figures
Update of
-
Antibiotics for acute otitis media in children.Cochrane Database Syst Rev. 2013 Jan 31;(1):CD000219. doi: 10.1002/14651858.CD000219.pub3. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2015 Jun 23;(6):CD000219. doi: 10.1002/14651858.CD000219.pub4. PMID: 23440776 Updated.
Comment in
-
Antibiotics administered for acute otitis media have modest benefits and adverse effects.Evid Based Med. 2016 Oct;21(5):181. doi: 10.1136/ebmed-2016-110398. Epub 2016 Aug 18. Evid Based Med. 2016. PMID: 27539210 No abstract available.
-
Antibiotics for Otitis Media in Children.Am Fam Physician. 2018 Jun 15;97(12):Online. Am Fam Physician. 2018. PMID: 30216004 No abstract available.
References
References to studies included in this review
Appelman 1991 {published data only}
-
- Claessen JQ, Appelman CL, Touw Otten FW, Melker RA, Hordijk GJ. Persistence of middle ear dysfunction after recurrent acute otitis media. Clinical Otolaryngology 1994;19:35‐40. - PubMed
Burke 1991 {published data only}
Damoiseaux 2000 {published data only}
Halsted 1968 {published data only}
-
- Halsted C, Lepow ML, Balassanian N, Emmerich J, Wolinsky E. Otitis media: clinical observation, microbiology and evaluation of therapy. American Journal of Diseases of Children 1968;115(5):542‐51. - PubMed
Hoberman 2011 {published data only}
Howie 1972 {published data only}
-
- Howie VM, Ploussard JH. Efficacy of fixed combination antibiotics versus separate components in otitis media: effectiveness of erythromycin estolate, triple sulfonamide, ampicillin, erythromycin estolate‐triple sulfonamide, and placebo in 280 patients with acute otitis media under two and one‐half years of age. Clinical Pediatrics 1972;11(4):205‐14. - PubMed
Kaleida 1991 {published data only}
-
- Kaleida PH, Casselhrant ML, Rockette HE, Paradise JL, Bluestone CD, Blatter MM, et al. Amoxicillin or myringotomy or both for acute otitis media: results of a randomized clinical trial. Paediatrics 1991;87(4):466‐74. - PubMed
Laxdal 1970 {published data only}
Le Saux 2005 {published data only}
-
- Saux N, Gaboury I, Baird M, Klassen TP, MacCormick J, Blanchard C, et al. A randomized, double‐blind, placebo‐controlled noninferiority trial of amoxicillin for clinically diagnosed acute otitis media in children 6 months to 5 years of age. Canadian Medical Association Journal 2005;172(3):335‐41. - PMC - PubMed
Little 2001 {published data only}
McCormick 2005 {published data only}
-
- McCormick DP, Chonmaitree T, Pittman C, Saeed K, Friedman NR, Uchida T, et al. Nonsevere acute otitis media: a clinical trial comparing outcomes of watchful waiting versus immediate antibiotic treatment. Pediatrics 2005;115(6):1455‐65. - PubMed
Mygind 1981 {published data only}
-
- Mygind N, Meistrup‐Larsen K‐I, Thomsen J, Thomsen VF, Josefsson K, Sorensen H. Penicillin in acute otitis media: a double‐blind placebo‐controlled trial. Clinical Otolaryngology 1981;6:5‐13. - PubMed
-
- Thomsen J, Meistrup‐Larsen KI, Sorensen H, Larsen PK, Mygind N. Penicillin and acute otitis: short and long term results. Annals of Otology, Rhinology and Laryngology, Supplement 1980;89:271‐4. - PubMed
Neumark 2007 {published data only}
Spiro 2006 {published data only}
-
- Spiro DM, Tay K, Arnold DH, Dziura J, Baker M, Shapiro ED. Wait‐and‐see prescription for the treatment of acute otitis media. JAMA 2006;296(10):1235‐41. - PubMed
Tähtinen 2011 {published data only}
-
- Tähtinen PA, Laine MK, Huovinen P, Jalava J, Ruuskanen O, Ruohola A. A placebo‐controlled trial of antimicrobial treatment for acute otitis media. New England Journal of Medicine 2011;364(2):116‐26. - PubMed
Tapiainen 2014 {published data only}
-
- Tapiainen T, Kujala T, Renko M, Koivunen P, Kontiokari T, Kristo A, et al. Effect of antimicrobial treatment of acute otitis media on the daily disappearance of middle ear effusion: a placebo‐controlled trial. JAMA Pediatrics 2014;168(7):635‐41. - PubMed
Thalin 1985 {published data only}
-
- Thalin A, Densert O, Larsson A, Lyden E, Ripa T. Is penicillin necessary in the treatment of acute otitis media?. Proceedings of the International Conference on Acute and Secretory Otitis Media 1985, Jerusalem. Amsterdam: Kugler Publications, 1985:441‐6.
van Buchem 1981a {published data only}
-
- Buchem FL, Dunk JHM, van't Hof MA. Therapy of acute otitis media: myringotomy, antibiotics or neither? A double‐blind study in children. Lancet 1981;2:883‐7. - PubMed
van Buchem 1981b {published data only}
-
- Buchem FL, Dunk JHM, van't Hof MA. Therapy of acute otitis media: myringotomy, antibiotics or neither? A double‐blind study in children. Lancet 1981;2:883‐7. - PubMed
References to studies excluded from this review
Arguedas 2011 {published data only}
-
- Arguedas A, Soley C, Kamicker BJ, Jorgensen DM. Single‐dose extended‐release azithromycin versus a 10‐day regimen of amoxicillin/clavulanate for the treatment of children with acute otitis media. International Journal of Infectious Diseases 2011;15(4):e240‐8. - PubMed
Casey 2012 {published data only}
Chaput 1982 {published data only}
Engelhard 1989 {published data only}
-
- Engelhard D, Strauss N, Jorczak‐Sarni L, Cohen D, Sacjs TG, Shapiro M. Randomised study of myringotomy, amoxycillin/clavulanate, or both for acute otitis media in infants. Lancet 1989;2(8655):141‐3. - PubMed
Liu 2011 {published data only}
Ostfeld 1987 {published data only}
-
- Ostfeld E, Segal J, Kaufstein M, Gelernter I. Management of acute otitis media without primary administration of systemic antimicrobial agents. Recent advances in otitis media. Proceedings of the Fourth International Symposium. Toronto: BC Decker, 1987:235‐9.
Rudberg 1954 {published data only}
-
- Rudberg RD. Acute otitis media: comparative therapeutic results of sulphonamide and penicillin administered in various forms. Acta Oto‐Laryngologica 1954;113(Suppl):1‐79. - PubMed
Ruohola 2003 {published data only}
-
- Ruohola A, Heikkinen T, Meurman O, Puhakka T, Lindblad N, Ruuskanen O. Antibiotic treatment of acute otorrhea through tympanostomy tube: randomized double‐blind placebo‐controlled study with daily follow‐up. Pediatrics 2003;111(5):1061‐7. - PubMed
Sarrell 2003 {published data only}
-
- Sarrell EM, Cohen HA, Kahan E. Naturopathic treatment for ear pain in children. Pediatrics 2003;111(5):574‐9. - PubMed
Tähtinen 2012 {published data only}
-
- Tähtinen PA, Laine MK, Ruuskanen O, Ruohola A. Delayed versus immediate antimicrobial treatment for acute otitis media. Pediatric Infectious Disease Journal 2012;31(12):1227‐32. - PubMed
References to ongoing studies
ACTRN12608000424303 {published data only}
-
- ACTRN12608000424303. Antibiotics for asymptomatic acute otitis media. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=1260... (accessed 26 November 2014).
Additional references
AAP 2013
-
- American Academy of Pediatrics, American Academy of Family Physicians. Clinical practice guidelines: diagnosis and management of acute otitis media. Pediatrics 2013;131(3):e964‐99. - PubMed
Akkerman 2005
-
- Akkerman AE, Kuyvenhoven MM, Wouden JC, Verhij TJM. Analysis of under‐and overprescribing of antibiotics in acute otitis media in general practice. Journal of Antimicrobial Chemotherapy 2005;56:569‐74. - PubMed
Arnold 2005
Arola 1990
-
- Arola M, Ruuskanen O, Ziegler T, Mertsola J, Näntö‐Salonen K, Putto‐Laurila A, et al. Clinical role of respiratory virus infection in acute otitis media. Pediatrics 1990;86:848‐55. - PubMed
Barkai 2009
-
- Barkai G, Leibovitz E, Givon‐Lavi N, Dagan R. Potential contribution by nontypable Haemophilus influenzae in protracted and recurrent acute otitis media. Pediatric Infectious Disease Journal 2009;28:466‐71. - PubMed
Berman 1995
-
- Berman S. Otitis media in developing countries. Pediatrics 1995;96:126‐31. - PubMed
Casey 2013
Cates 1999
-
- Cates C. An evidence based approach to reducing antibiotic use in children with acute otitis media: controlled before and after the study. BMJ 1999;318:715‐6. [The handout is available at http://www.cates.cwc.net/] - PMC - PubMed
Chao 2008
-
- Chao JH, Kunkov S, Reyes LB, Lichten S, Crain EF. Comparison of two approaches to observation therapy for acute otitis media in the emergency department. Pediatrics 2008;121:31352‐e6. - PubMed
Chonmaitree 1992
-
- Chonmaitree T, Owen MJ, Patel JA, Hedgpeth D, Horlick D, Howie VM. Effect of viral respiratory tract infection on outcome of acute otitis media. Journal of Pediatrics 1992;120:856‐62. - PubMed
Coker 2010
-
- Coker TR, Chan LS, Newberry SJ, Limbos MA, Suttorp MJ, Shekelle PG, et al. Diagnosis, microbial epidemiology, and antibiotic treatment of acute otitis media in children: a systematic review. JAMA 2010;304(19):2161‐9. - PubMed
Dickersin 1994
Froom 2001
-
- Froom J, Culpepper L, Green LA, Melker RA, Grob P, Heeren T, et al. A cross‐national study of acute otitis media: risk factors, severity, and treatment at initial visit. Report from the International Primary Care Network (IPCN) and the Ambulatory Sentinel Practice Network (ASPN). Journal of the American Board of Family Practice 2001;14:406‐17. - PubMed
Gillies 2014
-
- Gillies M, Ranakusuma A, Hoffmann T, Thorning S, McGuire T, Glasziou P, et al. Common harms from amoxicillin: a systematic review and meta‐analysis of randomized placebo‐controlled trials for any indication. Canadian Medical Association Journal 2014 Nov 17 [Epub ahead of print]:.. [DOI: 10.1503/cmaj.140848] - DOI - PMC - PubMed
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Klein 1989
-
- Klein JO. Epidemiology of otitis media. Pediatic Infectious Disease Journal 1989;8(Suppl 1):89. - PubMed
Koopman 2008
-
- Koopman L, Hoes AW, Glasziou PP, Appelman CL, Burke P, McCormick DP, et al. Antibiotic therapy to prevent the development of asymptomatic middle ear effusion in children with acute otitis media. Archives of Otolaryngology ‐ Head and Neck Surgery 2008;134(2):128‐32. - PubMed
Kozyrskyj 2010
Lefebvre 2011
-
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Little 2006
McCormick 2007
-
- McCormick DP, Chandler SM, Chonmaitree T. Laterality of acute otitis media: different clinical and microbiologic characteristics. Pediatric Infectious Disease Journal 2007;26:583‐8. - PubMed
Rosenfeld 1994
-
- Rosenfeld RM, Vertrees JE, Carr J, Cipolle RJ, Uden DL, Giebink GS, et al. Clinical efficacy of antimicrobial drugs for acute otitis media: meta‐analysis of 5400 children from thirty‐three randomized trials. Journal of Pediatrics 1994;124:355‐67. - PubMed
Rothman 2003
-
- Rothman R, Owens T, Simel D. Does this child have acute otitis media?. JAMA 2003;290(12):1633‐40. - PubMed
Rovers 2006
-
- Rovers MM, Glasziou P, Appelman CL, Burke P, McCormick DP, Damoiseaux RA, et al. Antibiotics for acute otitis media: a meta‐analysis with individual patient data. Lancet 2006;368:1429‐35. - PubMed
Spurling 2013
Stool 1989
-
- Stool SE, Field MJ. The impact of otitis media. Pediatic Infectious Disease Journal 1989;8(Suppl 1):11‐4. - PubMed
Teele 1989
-
- Teele DW, Klein JO, Rosner B. Epidemiology of otitis media during first seven years of life in children in greater Boston: a prospective cohort study. Journal of Infectious Diseases 1989;160:83‐94. - PubMed
References to other published versions of this review
Glasziou 1995
-
- Glasziou PP, Hayem M, Mar CB. A meta‐analysis of treatments for acute otitis media: antibiotic vs placebo, short vs long antibiotic course, and myringotomy. Cochrane Database of Systematic Reviews 1995, Issue 1. [DOI: 10.1002/14651858.CD000219] - DOI
Glasziou 1997
Glasziou 1999
-
- Glasziou PP, Hayem M, Mar CB. Antibiotics versus placebo for acute otitis media in children. Cochrane Database of Systematic Reviews 1999, Issue 3. [DOI: 10.1002/14651858.CD000219.pub2] - DOI
Glasziou 2005
Sanders 2009
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous