

Usefulness of data from magnetic resonance imaging to improve prediction of dementia: population based cohort study
- PMID: 26099688
- PMCID: PMC4476487
- DOI: 10.1136/bmj.h2863
Usefulness of data from magnetic resonance imaging to improve prediction of dementia: population based cohort study
Abstract
Objective: To determine whether the addition of data derived from magnetic resonance imaging (MRI) of the brain to a model incorporating conventional risk variables improves prediction of dementia over 10 years of follow-up.
Design: Population based cohort study of individuals aged ≥ 65.
Setting: The Dijon magnetic resonance imaging study cohort from the Three-City Study, France.
Participants: 1721 people without dementia who underwent an MRI scan at baseline and with known dementia status over 10 years' follow-up.
Main outcome measure: Incident dementia (all cause and Alzheimer's disease).
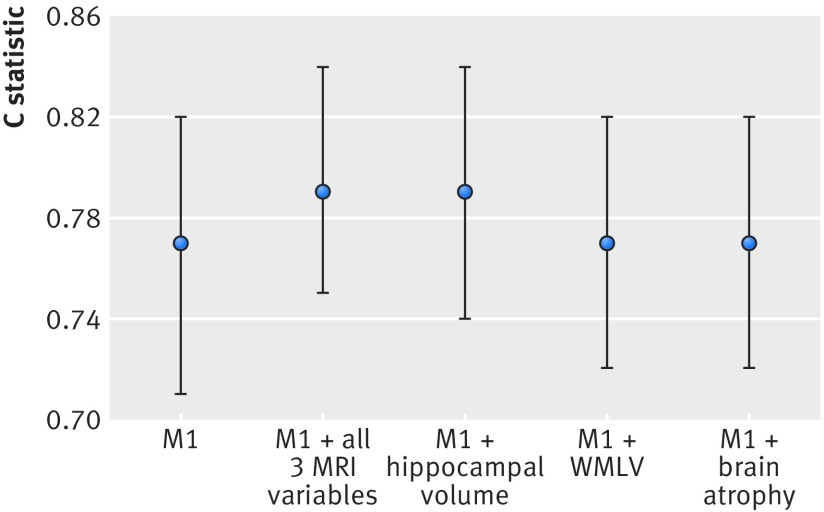
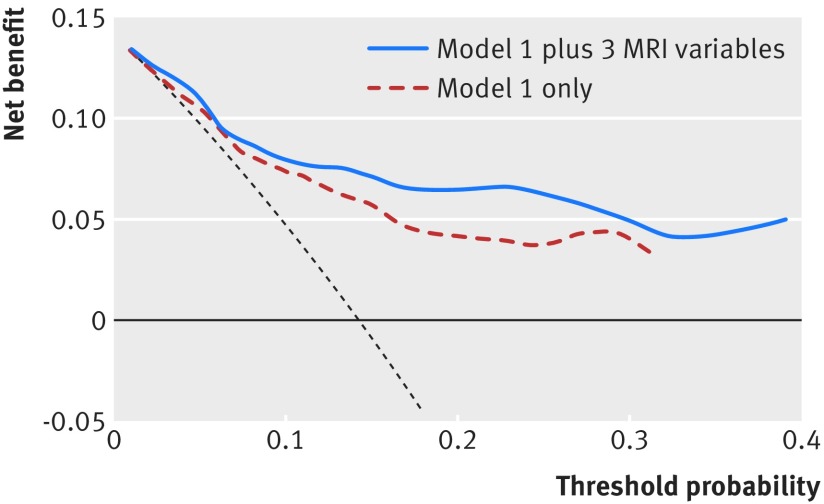
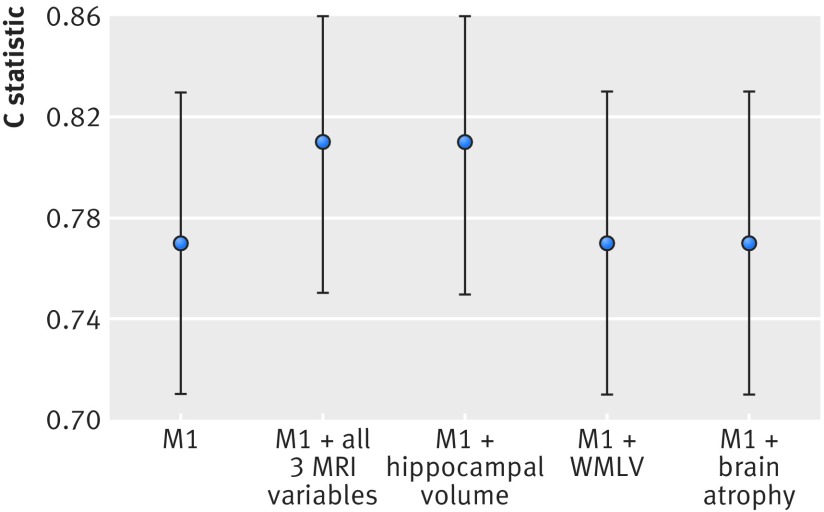
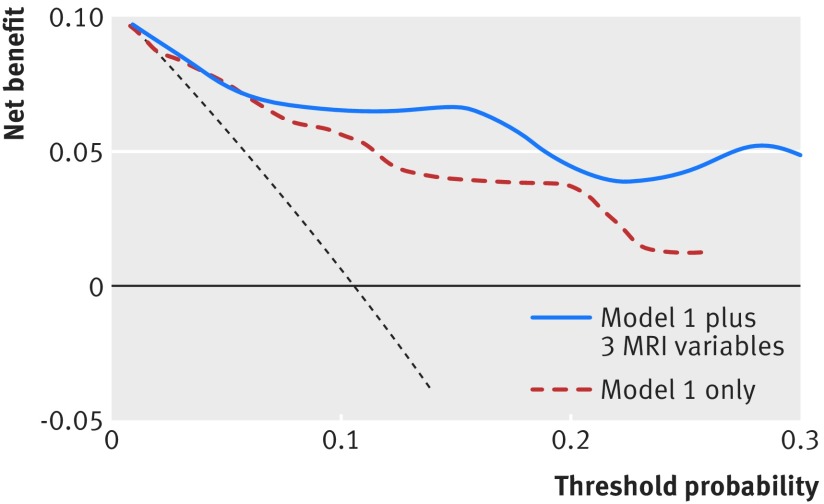
Results: During 10 years of follow-up, there were 119 confirmed cases of dementia, 84 of which were Alzheimer's disease. The conventional risk model incorporated age, sex, education, cognition, physical function, lifestyle (smoking, alcohol use), health (cardiovascular disease, diabetes, systolic blood pressure), and the apolipoprotein genotype (C statistic for discrimination performance was 0.77, 95% confidence interval 0.71 to 0.82). No significant differences were observed in the discrimination performance of the conventional risk model compared with models incorporating data from MRI including white matter lesion volume (C statistic 0.77, 95% confidence interval 0.72 to 0.82; P=0.48 for difference of C statistics), brain volume (0.77, 0.72 to 0.82; P=0.60), hippocampal volume (0.79, 0.74 to 0.84; P=0.07), or all three variables combined (0.79, 0.75 to 0.84; P=0.05). Inclusion of hippocampal volume or all three MRI variables combined in the conventional model did, however, lead to significant improvement in reclassification measured by using the integrated discrimination improvement index (P=0.03 and P=0.04) and showed increased net benefit in decision curve analysis. Similar results were observed when the outcome was restricted to Alzheimer's disease.
Conclusions: Data from MRI do not significantly improve discrimination performance in prediction of all cause dementia beyond a model incorporating demographic, cognitive, health, lifestyle, physical function, and genetic data. There were, however, statistical improvements in reclassification, prognostic separation, and some evidence of clinical utility.
© Stephan et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Predicting dementia.BMJ. 2015 Jun 22;350:h2994. doi: 10.1136/bmj.h2994. BMJ. 2015. PMID: 26099820 No abstract available.
-
[MRI does not improve the prediction of dementia].MMW Fortschr Med. 2015 Nov 12;157 Spec No 2:46. doi: 10.1007/s15006-015-3787-6. MMW Fortschr Med. 2015. PMID: 26953474 German. No abstract available.
References
-
- Alzheimer’s Disease International. World Alzheimer Report. 2009. www.alz.co.uk/research/files/WorldAlzheimerReport.pdf.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical