

Glucocorticosteroids for sepsis: systematic review with meta-analysis and trial sequential analysis
- PMID: 26100123
- PMCID: PMC4483251
- DOI: 10.1007/s00134-015-3899-6
Glucocorticosteroids for sepsis: systematic review with meta-analysis and trial sequential analysis
Abstract
Introduction: Glucocorticosteroids (steroids) are widely used for sepsis patients. However, the potential benefits and harms of both high and low dose steroids remain unclear. A systematic review of randomised clinical trials with meta-analysis and trial sequential analysis (TSA) might shed light on this clinically important question.
Methods: A systematic review was conducted according to a published protocol and The Cochrane Handbook methodology including meta-analyses, TSA of randomised clinical trials, and external validity estimation (GRADE). Randomised clinical trials evaluating steroids were included for sepsis patients (systemic inflammatory response syndrome, sepsis, severe sepsis or septic shock) aged >18 years. Cochrane Central Register of Controlled Trials (CENTRAL), PubMed/Medline, Embase, Web of Science and Cinahl were searched until 18 February 2015. No language restrictions were applied. Primary outcomes were mortality at longest follow-up and serious adverse events.
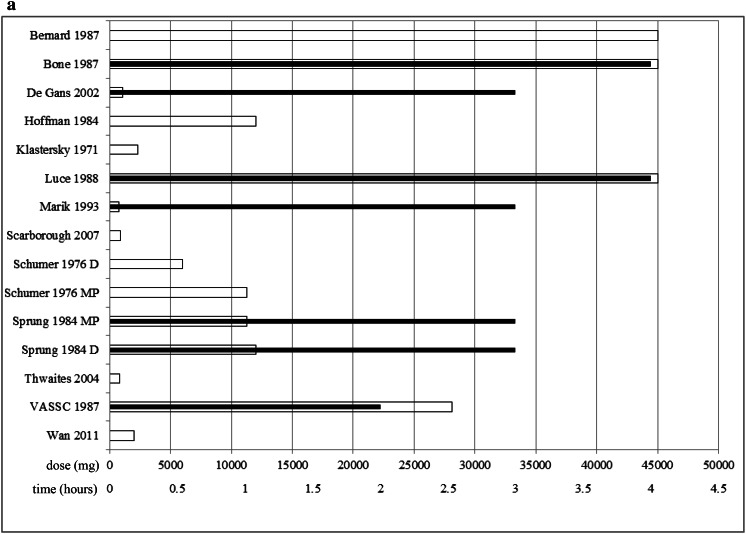
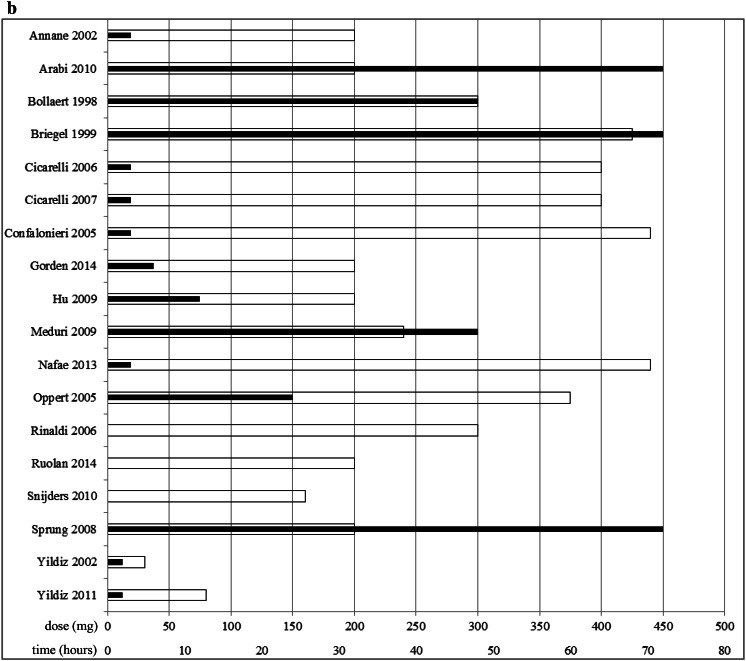
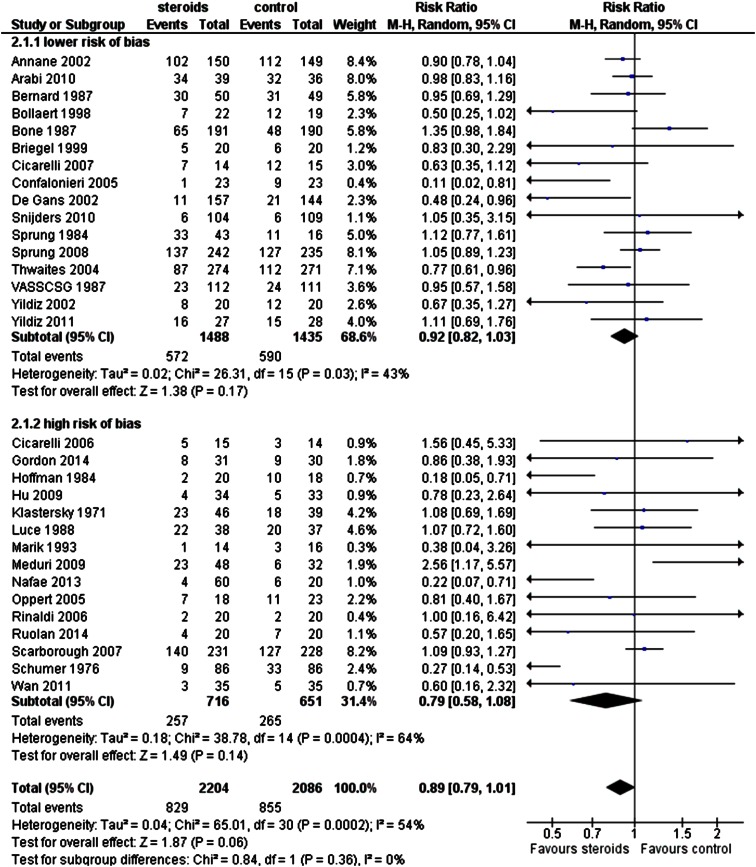
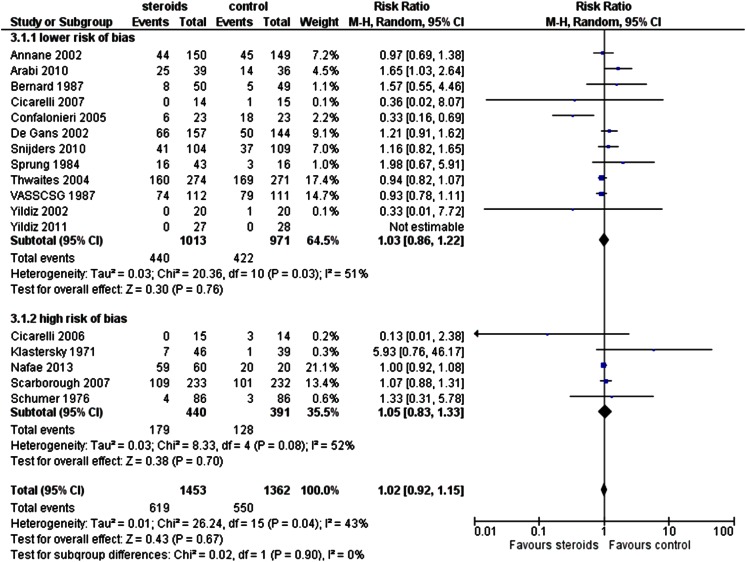
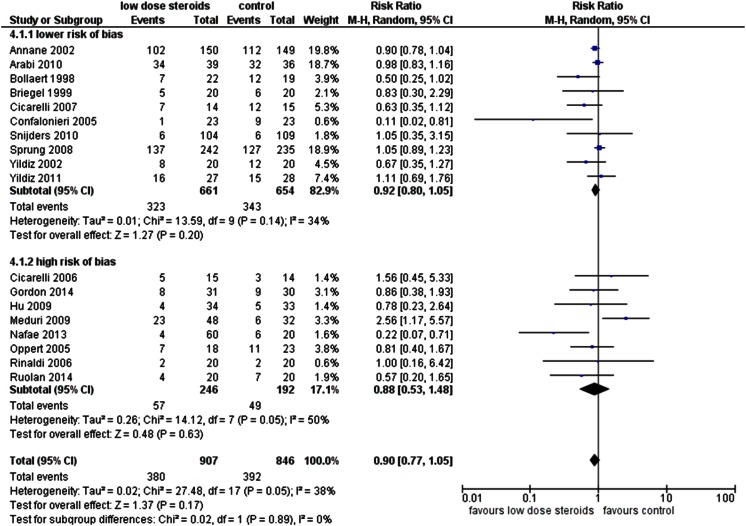
Results: A total of 35 trials randomising 4682 patients were assessed and reviewed in full text. All trials but two had high risk of bias. No statistically significant effect was found for any dose of steroids versus placebo or no intervention on mortality at maximal follow-up [relative risk (RR) 0.89; TSA adjusted confidence interval (CI) 0.74-1.08]. Two trials with low risk of bias also showed no statistically significant difference (random-effects model RR 0.38, 95% CI 0.06-2.42). Similar results were obtained in subgroups of trials stratified according to high (>500 mg) or low (≤ 500 mg) dose hydrocortisone (or equivalent) (RR 0.87; TSA-adjusted CI 0.38-1.99; and RR 0.90; TSA-adjusted CI 0.49-1.67, respectively). There were also no statistically significant effects on serious adverse events other than mortality (RR 1.02; TSA-adjusted CI 0.7-1.48). The effects did not vary according to the degree of sepsis. TSA showed that many more randomised patients are needed before definitive conclusions may be drawn.
Conclusion: Evidence to support or negate the use of steroids in any dose in sepsis patients is lacking. The results of ongoing and future well-designed, large randomised clinical trials are needed.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
