

Primary Care Medication Safety Surveillance with Integrated Primary and Secondary Care Electronic Health Records: A Cross-Sectional Study
- PMID: 26100143
- PMCID: PMC4486763
- DOI: 10.1007/s40264-015-0304-x
Primary Care Medication Safety Surveillance with Integrated Primary and Secondary Care Electronic Health Records: A Cross-Sectional Study
Abstract
Introduction: The extent of preventable medication-related hospital admissions and medication-related issues in primary care is significant enough to justify developing decision support systems for medication safety surveillance. The prerequisite for such systems is defining a relevant set of medication safety-related indicators and understanding the influence of both patient and general practice characteristics on medication prescribing and monitoring.
Objective: The aim of the study was to investigate the feasibility of linked primary and secondary care electronic health record data for surveillance of medication safety, examining not only prescribing but also monitoring, and associations with patient- and general practice-level characteristics.
Methods: A cross-sectional study was conducted using linked records of patients served by one hospital and over 50 general practices in Salford, UK. Statistical analysis consisted of mixed-effects logistic models, relating prescribing safety indicators to potential determinants.
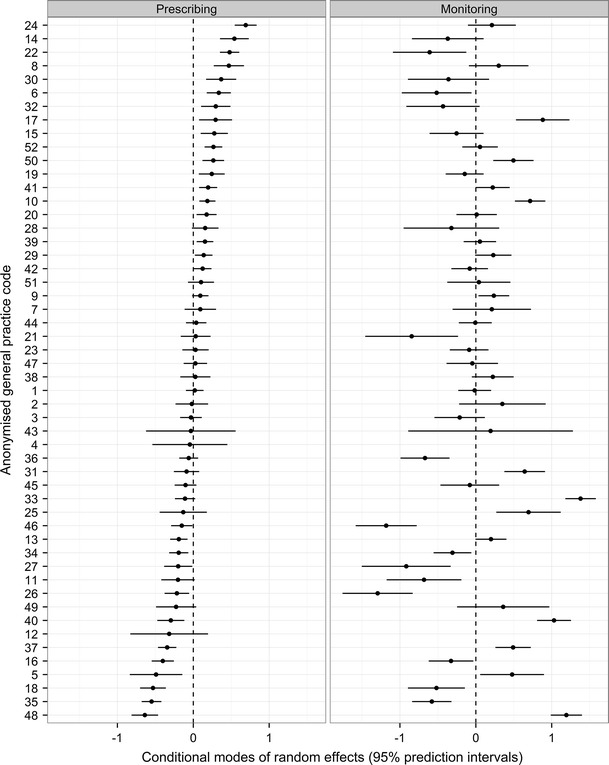
Results: The overall prevalence (proportion of patients with at least one medication safety hazard) was 5.45 % for prescribing indicators and 7.65 % for monitoring indicators. Older patients and those on multiple medications were at higher risk of prescribing hazards, but at lower risk of missed monitoring. The odds of missed monitoring among all patients were 25 % less for males, 50 % less for patients in practices that provide general practitioner training, and threefold higher in practices serving the most deprived compared with the least deprived areas. Practices with more prescribing hazards did not tend to show more monitoring issues.
Conclusions: Systematic collection, collation, and analysis of linked primary and secondary care records produce plausible and useful information about medication safety for a health system. Medication safety surveillance systems should pay close attention to patient age and polypharmacy with respect to both prescribing and monitoring failures; treat prescribing and monitoring as different statistical processes, rather than a combined measure of prescribing safety; and audit the socio-economic equity of missed monitoring.
Figures


References
-
- Galvin R, Moriarty F, Cousins G, Cahir C, Motterlini N, Bradley M, et al. Prevalence of potentially inappropriate prescribing and prescribing omissions in older Irish adults: findings from The Irish LongituDinal Study on Ageing study (TILDA) Eur J Clin Pharmacol. 2014;70:599–606. doi: 10.1007/s00228-014-1651-8. - DOI - PMC - PubMed
-
- Schubert I, Küpper-Nybelen J, Ihle P, Thürmann P. Prescribing potentially inappropriate medication (PIM) in Germany’s elderly as indicated by the PRISCUS list. An analysis based on regional claims data: prescribing potentially inappropriate medication. Pharmacoepidemiol Drug Saf. 2013;22:719–727. doi: 10.1002/pds.3429. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
