

Initial thrombolysis treatment compared with anticoagulation for acute intermediate-risk pulmonary embolism: a meta-analysis
- PMID: 26101636
- PMCID: PMC4454855
- DOI: 10.3978/j.issn.2072-1439.2015.04.51
Initial thrombolysis treatment compared with anticoagulation for acute intermediate-risk pulmonary embolism: a meta-analysis
Abstract
Background: The use of thrombolysis in patients with acute, intermediate-risk pulmonary embolism (PE) remains controversial. This meta-analysis compared the efficacy and safety of thrombolysis and anticoagulation treatments for intermediate-risk PE patients.
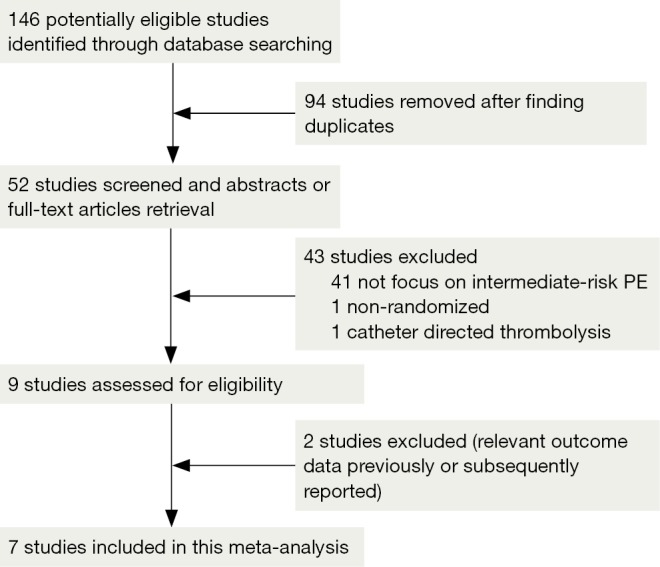
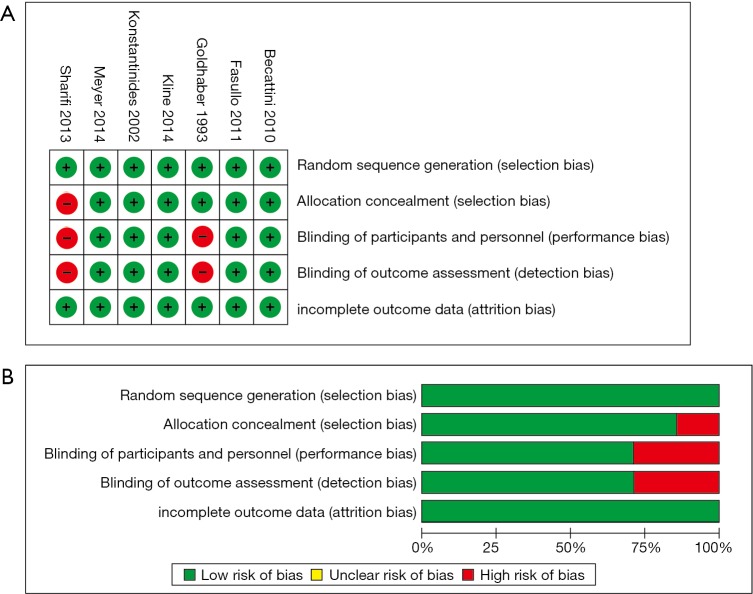
Methods: Two investigators independently reviewed the literature and collected data from randomized controlled trials (RCTs) of thrombolysis for intermediate-risk PE in the PubMed, MEDLINE, EMBASE, the Cochrane Library, and Chinese Biomedical Literature Databases (CBM).
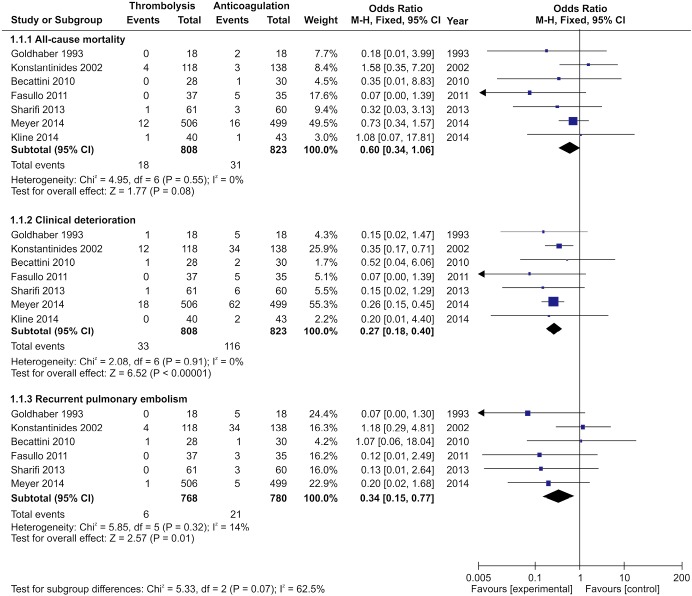
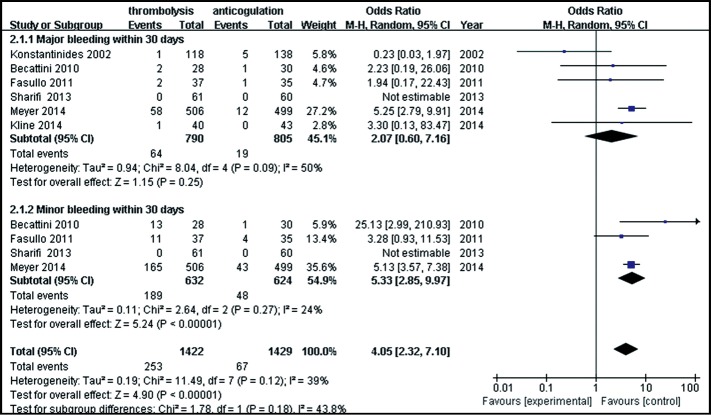
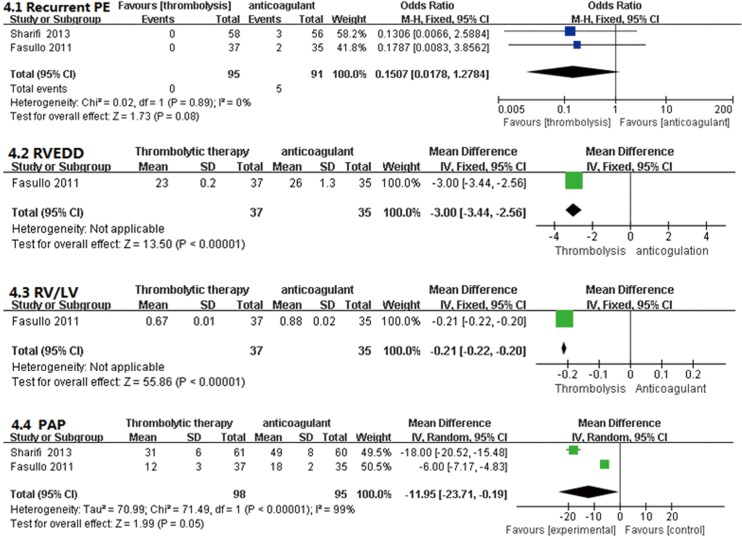
Results: A total of 1,631 intermediate-risk PE patients from seven studies were included. Significant differences were not found regarding the 30-day, all-cause mortality rates between the thrombolytic and anticoagulant groups [odds ratio (OR), 0.60; 95% confident interval (CI), 0.34-1.06; P=0.08]. The rate of clinical deterioration in the thrombolytic group was lower than that in the anticoagulant group (OR, 0.27; 95% CI, 0.18-0.41; P<0.01). Recurrent PE in the thrombolytic group was also significantly lower than that in the anticoagulant group (OR, 0.34; 95% CI, 0.15-0.77; P=0.01). Comparing the thrombolytic and anticoagulation groups, the incidence of minor bleeding was significantly higher in the thrombolytic group (OR, 5.33; 95% CI, 2.85-9.97; P<0.00001), but there were no difference in the incidences of major bleeding events (OR, 2.07; 95% CI, 0.60-7.16; P=0.25).
Conclusions: Thrombolytic treatment for intermediate-risk PE patients, if not contraindicated, could reduce clinical deterioration and recurrence of PE, and trends towards a decrease in all-cause, 30-day mortality. Despite thrombolytic treatment having an increased total bleeding risk, there was no difference in the incidence of major bleeding events, compared with patients receiving anticoagulation treatment.
Keywords: Thrombolytic therapy; anticoagulation treatment; efficacy; pulmonary embolism (PE); safety.
Figures
References
-
- Naess IA, Christiansen SC, Romundstad P, et al. Incidence and mortality of venous thrombosis: a population-based study. J Thromb Haemost 2007;5:692-9. - PubMed
-
- Goldhaber SZ. Venous thromboembolism: epidemiology and magnitude of the problem. Best Pract Res Clin Haematol 2012;25:235-42. - PubMed
-
- Cohen AT, Agnelli G, Anderson FA, et al. Venous thromboembolism (VTE) in Europe. The number of VTE events and associated morbidity and mortality. Thromb Haemost 2007;98:756-64. - PubMed
LinkOut - more resources
Full Text Sources