

IDENTIFICATION OF FLUID ON OPTICAL COHERENCE TOMOGRAPHY BY TREATING OPHTHALMOLOGISTS VERSUS A READING CENTER IN THE COMPARISON OF AGE-RELATED MACULAR DEGENERATION TREATMENTS TRIALS
- PMID: 26102433
- PMCID: PMC4479420
- DOI: 10.1097/IAE.0000000000000483
IDENTIFICATION OF FLUID ON OPTICAL COHERENCE TOMOGRAPHY BY TREATING OPHTHALMOLOGISTS VERSUS A READING CENTER IN THE COMPARISON OF AGE-RELATED MACULAR DEGENERATION TREATMENTS TRIALS
Abstract
Purpose: To examine treatment decisions by ophthalmologists versus reading center fluid identification from optical coherence tomography in Comparison of Age-Related Macular Degeneration Treatments Trials (CATT).
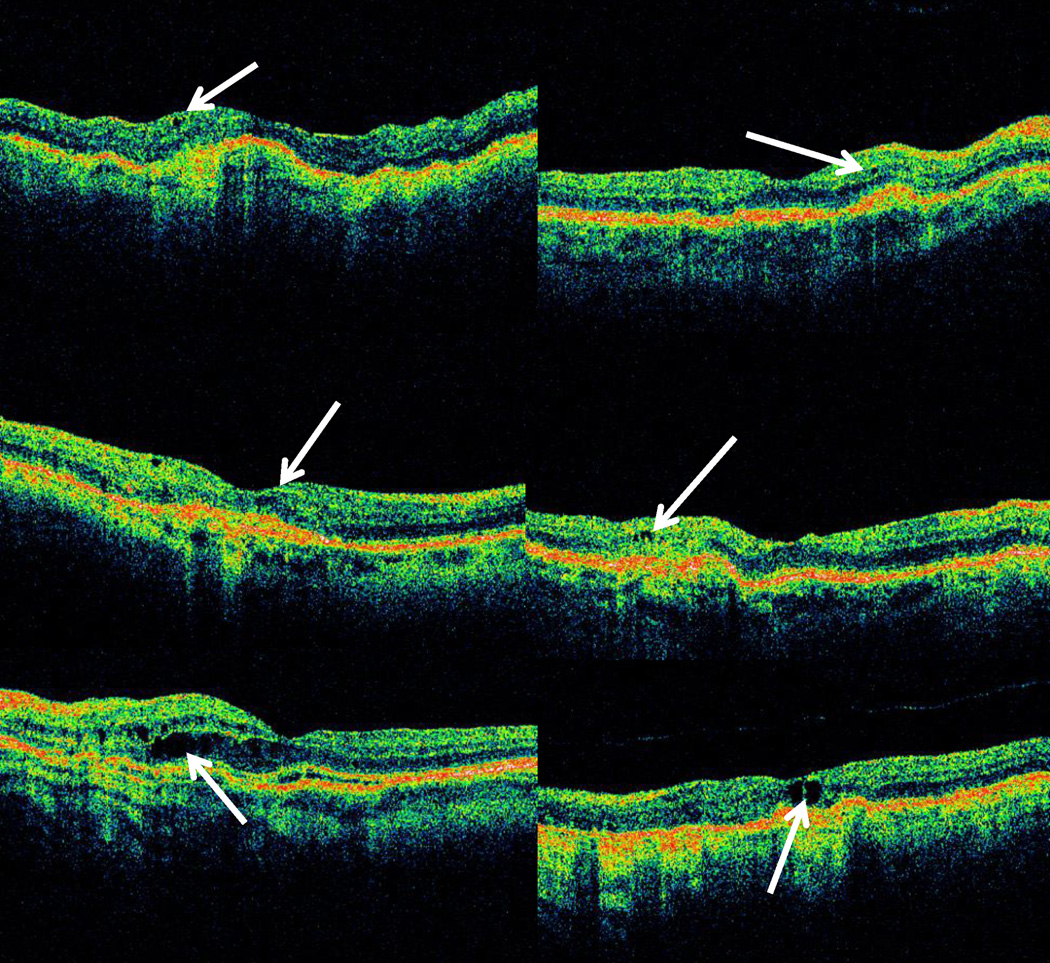
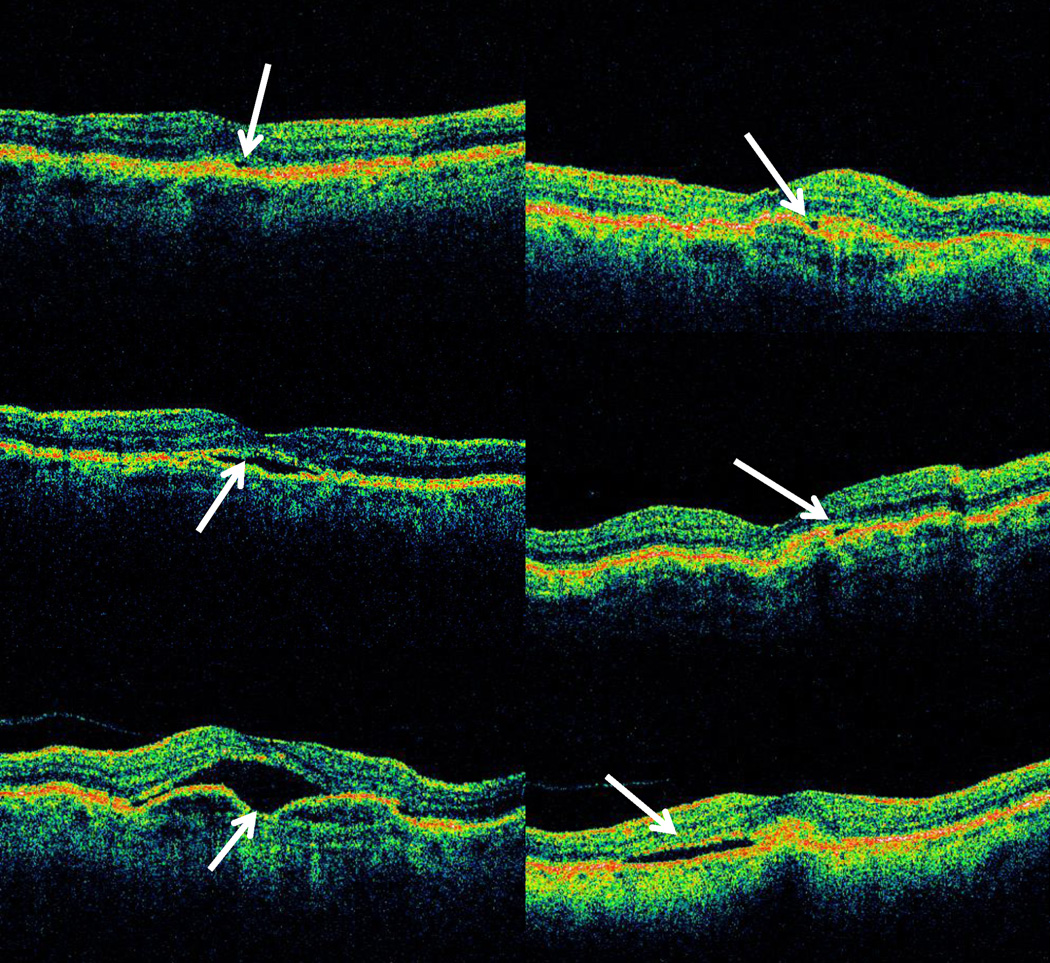
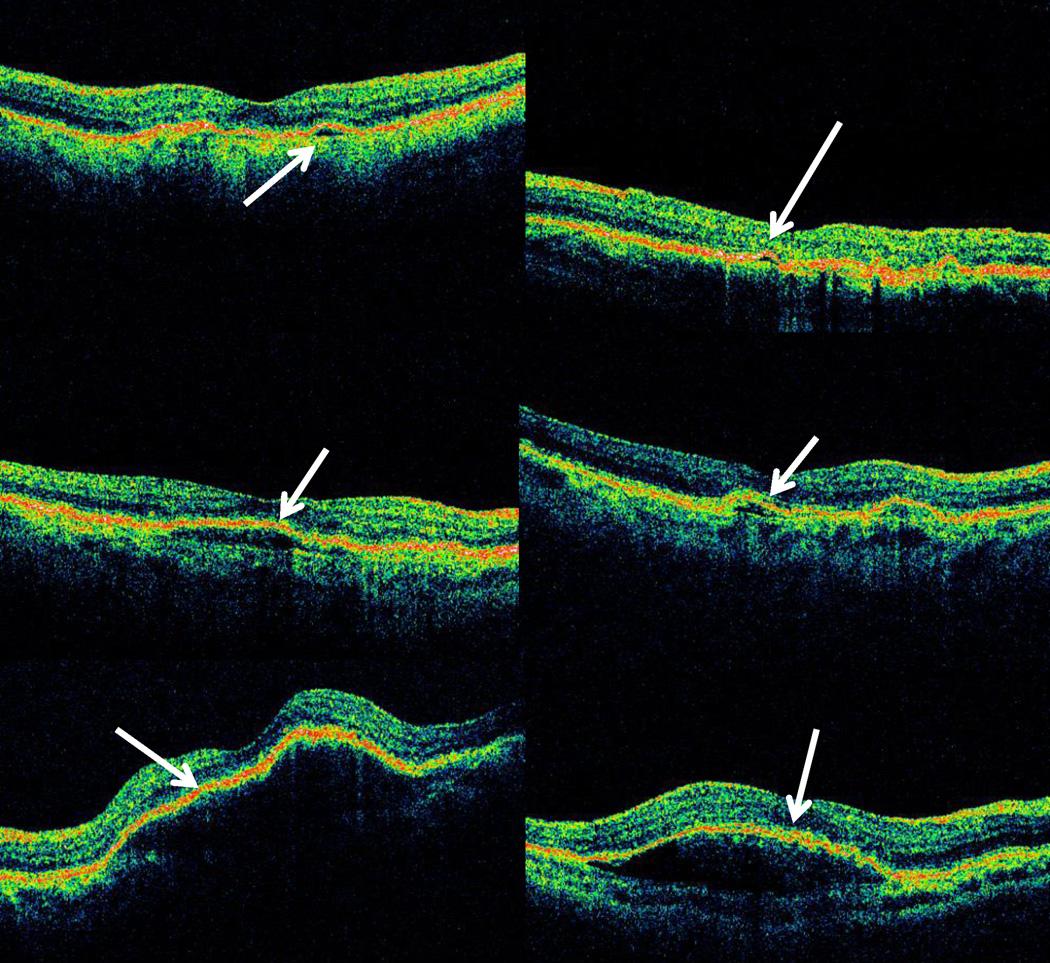
Methods: Fluid in 6,210 optical coherence tomography scans (598 patients) in "as needed treatment" arm of CATT Year 1 was compared with ophthalmologist's treatment: positive fluid agreement (PFA, fluid+, treatment+) and positive fluid discrepancy (PFD, fluid+, treatment-), negative fluid agreement (fluid-, treatment-) and negative fluid discrepancy (fluid-, treatment+). For PFDs, fluid location and visual acuity were characterized.
Results: Treatment and reading center fluid determination agreed in 72.1% (53.0% PFA, 19.1% negative fluid agreement) and disagreed in 27.9% (25.7% PFD, 2.2% negative fluid discrepancy) of visits, with no discrepancies for 20.9% of patients. Compared with PFA, PFD occurred more commonly with lower total foveal thickness (mean ± SD: 265 ± 103 PFD, 366 ± 151 μm PFA), presence of intraretinal fluid only, smaller fluid areas (PFA areas greater than twice those of PFD, P < 0.001), and greater decrease in retinal and lesion thickness. Mean acuities before, at, and after PFD were 65.8, 66.9, and 66.3 letters.
Conclusion: Treatment decisions by ophthalmologists matched reading center fluid determination in the majority of visits. More pronounced response to treatment and smaller foci of fluid likely contributed to PFD. Positive fluid discrepancy did not have substantial impact on subsequent visual acuity.
Figures
References
-
- Hee MR, Baumal CR, Puliafito CA, et al. Optical coherence tomography of age-related macular degeneration and choroidal neovascularization. Ophthalmology. 1996;103(8):1260–1270. - PubMed
-
- Ting TD, Oh M, Cox TA, et al. Decreased visual acuity associated with cystoid macular edema in neovascular age-related macular degeneration. Arch Ophthalmol. 2002;120(6):731–737. - PubMed
-
- Rahman W, Chen FK, Yeoh J, da Cruz L. Enhanced depth imaging of the choroid in patients with neovascular age-related macular degeneration treated with anti-VEGF therapy versus untreated patients. Graefes Arch Clin Exp Ophthalmol. 2012 - PubMed
-
- Gupta OP, Shienbaum G, Patel AH, et al. A Treat and Extend Regimen Using Ranibizumab for Neovascular Age-Related Macular Degeneration Clinical and Economic Impact. Ophthalmology - PubMed
-
- Dadgostar H, Ventura AA, Chung JY, et al. Evaluation of injection frequency and visual acuity outcomes for ranibizumab monotherapy in exudative age-related macular degeneration. Ophthalmology. 2009;116(9):1740–1747. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
