

Cost-Effectiveness of Collaborative Care for Depression in HIV Clinics
- PMID: 26102447
- PMCID: PMC4626259
- DOI: 10.1097/QAI.0000000000000732
Cost-Effectiveness of Collaborative Care for Depression in HIV Clinics
Abstract
Objective: To examine the cost-effectiveness of the HIV Translating Initiatives for Depression Into Effective Solutions (HITIDES) intervention.
Design: Randomized controlled effectiveness and implementation trial comparing depression collaborative care with enhanced usual care.
Setting: Three Veterans Health Administration HIV clinics in the Southern United States.
Subjects: Two hundred forty-nine HIV-infected patients completed the baseline interview; 123 were randomized to the intervention and 126 to usual care.
Intervention: HITIDES consisted of an offsite HIV depression care team that delivered up to 12 months of collaborative care. The intervention used a stepped-care model for depression treatment, and specific recommendations were based on the Texas Medication Algorithm Project and the VA/Department of Defense Depression Treatment Guidelines.
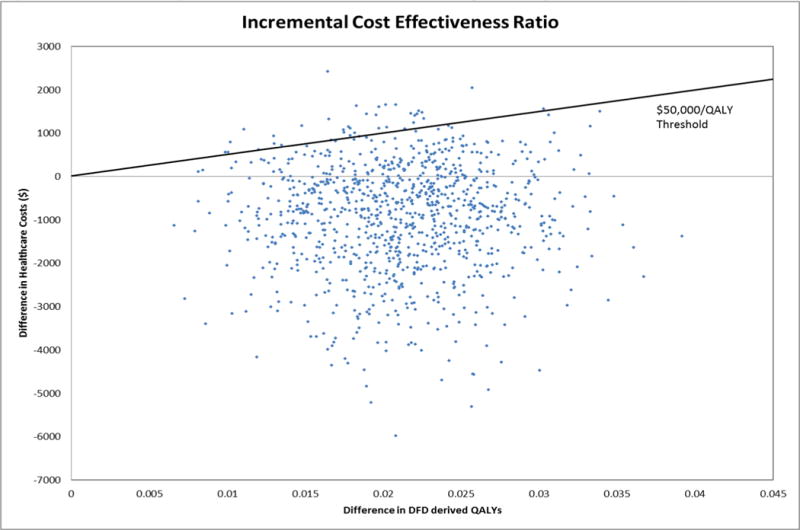
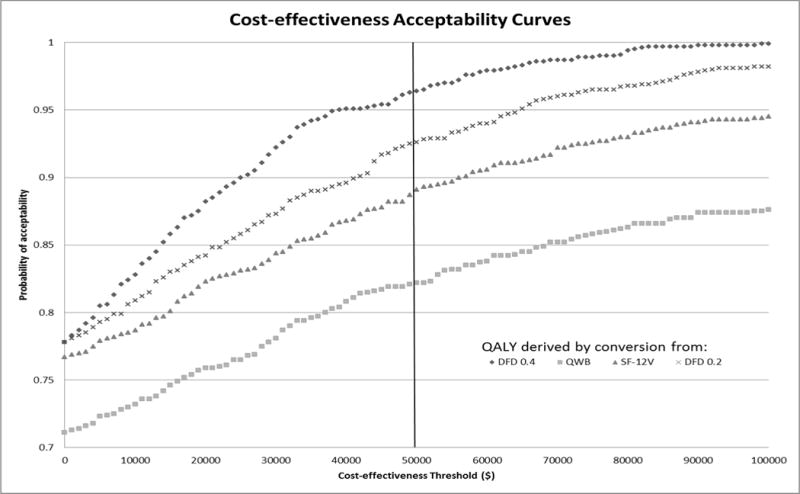
Main outcome measures: Quality-adjusted life years (QALYs) were calculated using the 12-Item Short Form Health Survey, the Quality of Well Being Scale, and by converting depression-free days to QALYs. The base case analysis used outpatient, pharmacy, patient, and intervention costs. Cost-effectiveness was calculated using incremental cost-effectiveness ratios (ICERs) and net health benefit. ICER distributions were generated using nonparametric bootstrap with replacement sampling.
Results: The HITIDES intervention was more effective and cost saving compared with usual care in 78% of bootstrapped samples. The intervention net health benefit was positive and therefore deemed cost-effective using an ICER threshold of $50,000/QALY.
Conclusions: In HIV clinic settings, this intervention was more effective and cost saving compared with usual care. Implementation of offsite depression collaborative care programs in specialty care settings may be a strategy that not only improves outcomes for patients but also maximizes the efficient use of limited health care resources.
Conflict of interest statement
Figures
References
-
- Robinson WD, Geske JA, Prest LA, Barnacle R. Depression treatment in primary care. The Journal of the American Board of Family Practice. 2005;18:79–86. - PubMed
-
- Katon W, Von Korff M, Lin E, Simon G, Walker E, Unutzer J, et al. Stepped collaborative care for primary care patients with persistent symptoms of depression: a randomized trial. Arch Gen Psychiatry. 1999;56:1109–1115. - PubMed
-
- Katon W, Robinson P, Von Korff M, Lin E, Bush T, Ludman E, et al. A multifaceted intervention to improve treatment of depression in primary care. Arch Gen Psychiatry. 1996;53:924–932. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
