

The Impact of Subclinical Disease and Mechanism of Detection on the Rise in Thyroid Cancer Incidence: A Population-Based Study in Olmsted County, Minnesota During 1935 Through 2012
- PMID: 26103159
- PMCID: PMC4560845
- DOI: 10.1089/thy.2014.0594
The Impact of Subclinical Disease and Mechanism of Detection on the Rise in Thyroid Cancer Incidence: A Population-Based Study in Olmsted County, Minnesota During 1935 Through 2012
Abstract
Background: An ongoing epidemic of thyroid carcinoma (TC) has affected Americans since 1975. Understanding the contribution of subclinical disease and the mechanism of such disease detection may help to alter the course of this epidemic.
Methods: We used Rochester Epidemiology Project resources to examine the incidence of TC cases, disease specific mortality, and method of diagnosis during 1935 through 2012. During 2000-2012, we also extracted the mechanism of detection of clinically occult tumors.
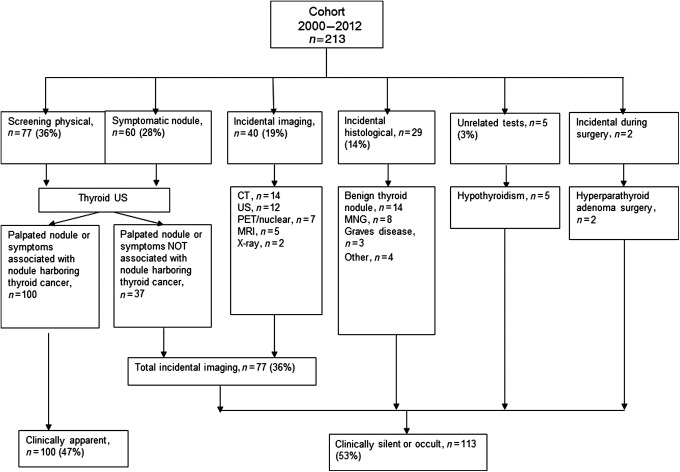
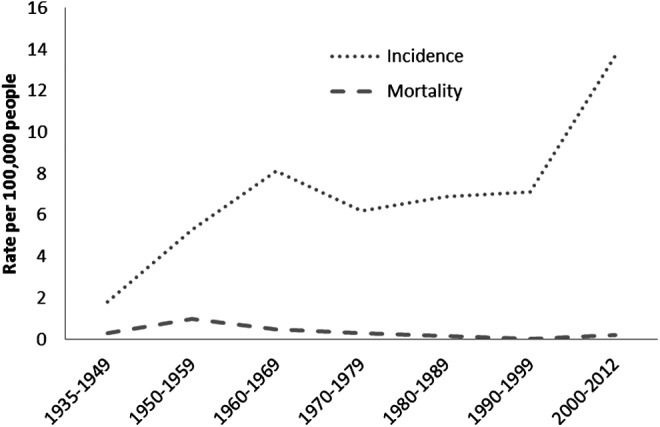
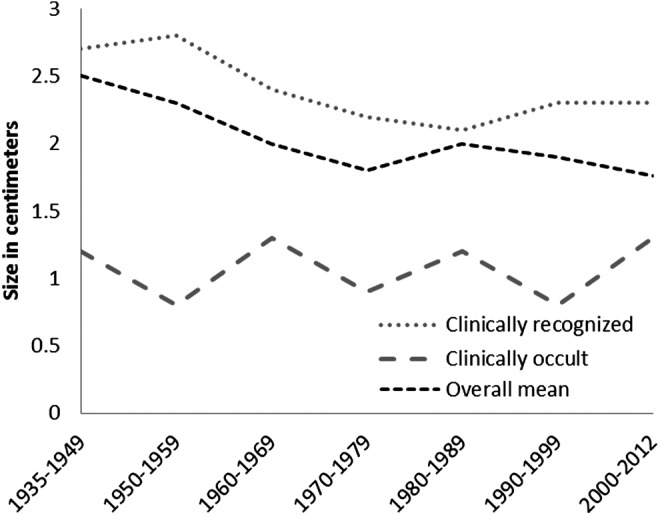
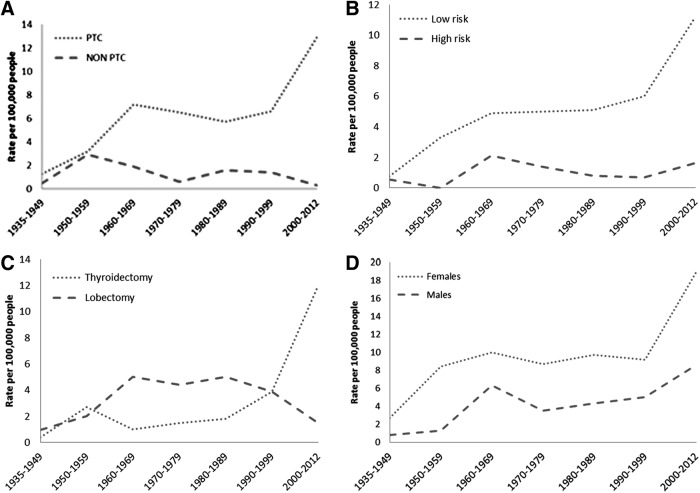
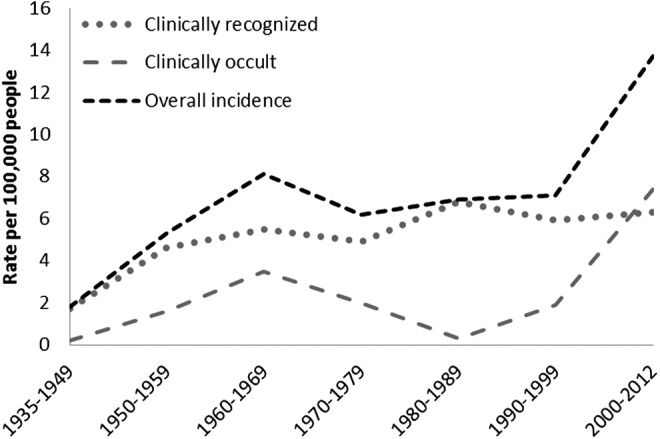
Results: The age-adjusted incidence (AAI) for TC increased from 7.1 [95% confidence interval (CI) 5.5-8.8] per 100,000 person-years (p-y) during 1990-1999 to 13.7 [CI 11.8-15.6] per 100,000 p-y during 2000-2012, with no change in disease-specific mortality since 1935. The incidence trend analysis stratified by the mechanism of detection revealed the AAI of clinically recognized TC was 5.5 per 100,000 p-y [CI 3.4-7.5] in 1960-1969, a rate similar to the incidence seen during 2000-2012. However, AAI of clinically occult TC increased from 0.2 per 100,000 p-y [CI 0.0-0.6] in 1935-1949 to 1.9 per 100,000 p-y [CI 1.2-2.9] in 1990-1999 and to 7.4 per 100,000 p-y [CI 6.0-8.8] in 2000-2012. During 2000-2012, the most frequent reasons for recognition of "occult" tumors were (1) incidental discovery during diagnostic neck imaging in 40 (19%), (2) pathology review of specimens from thyroid surgery for benign conditions in 29 (14%), and (3) investigations of patients with symptoms or palpable nodules that were clearly not associated with coexistent but occult TC but triggered the use of diagnostic neck imaging in 37 (27%).
Conclusions: In this population-based study conducted in Olmsted County, Minnesota, the rapid increased incidence of TC during 2000-2012 can be completely attributed to the increased diagnosis of occult TCs, which are mainly found through the use of diagnostic neck imaging. The incidence of clinical TC and disease-specific TC mortality remains stable since 1970, implying that the observed increased incidence is due to the increased detection of subclinical lesions.
Figures
References
-
- Davies L, Welch H. 2014. CUrrent thyroid cancer trends in the United States. JAMA Otolaryngol Head Neck Surg 140:317–322 - PubMed
-
- Aschebrook-Kilfoy B, Schechter RB, Shih YC, Kaplan EL, Chiu BC, Angelos P, Grogan RH. 2013. The clinical and economic burden of a sustained increase in thyroid cancer incidence. Cancer Epidemiol Biomarkers Prev 22:1252–1259 - PubMed
-
- Ito Y, Miyauchi A, Inoue H, Fukushima M, Kihara M, Higashiyama T, Tomoda C, Takamura Y, Kobayashi K, Miya A. 2010. An observational trial for papillary thyroid microcarcinoma in Japanese patients. World J Surg 34:28–35 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
