

Individual-patient meta-analysis of three randomized trials comparing endovascular versus open repair for ruptured abdominal aortic aneurysm
- PMID: 26104471
- PMCID: PMC4744980
- DOI: 10.1002/bjs.9852
Individual-patient meta-analysis of three randomized trials comparing endovascular versus open repair for ruptured abdominal aortic aneurysm
Abstract
Background: The benefits of endovascular repair of ruptured abdominal aortic aneurysm remain controversial, without any strong evidence about advantages in specific subgroups.
Methods: An individual-patient data meta-analysis of three recent randomized trials of endovascular versus open repair of abdominal aortic aneurysm was conducted according to a prespecified analysis plan, reporting on results to 90 days after the index event.
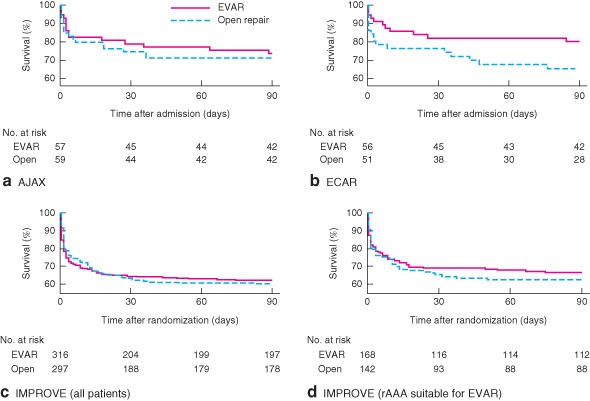
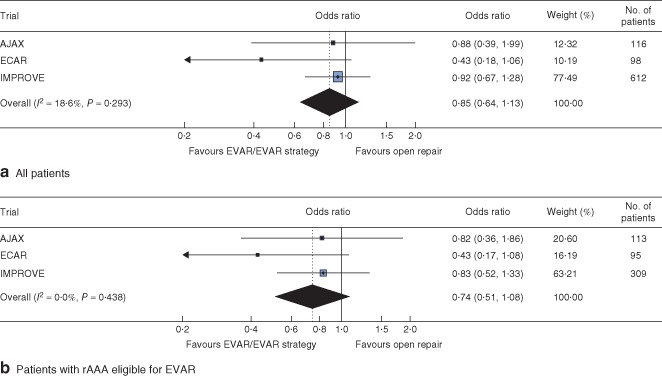
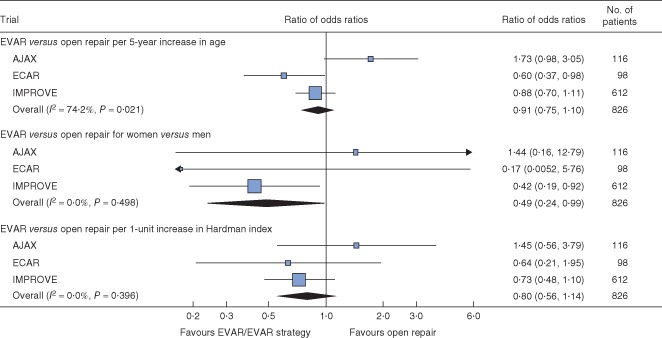
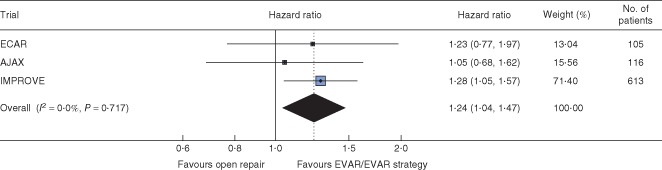
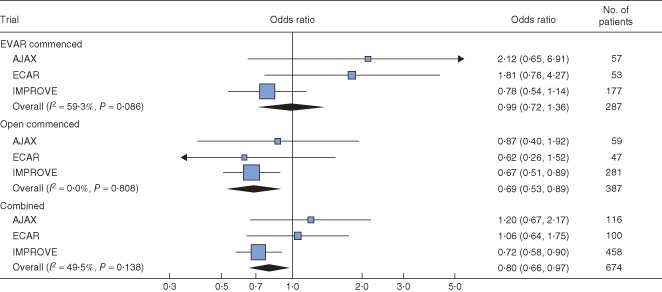
Results: The trials included a total of 836 patients. The mortality rate across the three trials was 31.3 per cent for patients randomized to endovascular repair/strategy and 34.0 per cent for those randomized to open repair at 30 days (pooled odds ratio 0.88, 95 per cent c.i. 0.66 to 1.18), and 34.3 and 38.0 per cent respectively at 90 days (pooled odds ratio 0.85, 0.64 to 1.13). There was no evidence of significant heterogeneity in the odds ratios between trials. Mean(s.d.) aneurysm diameter was 8.2(1.9) cm and the overall in-hospital mortality rate was 34.8 per cent. There was no significant effect modification with age or Hardman index, but there was indication of an early benefit from an endovascular strategy for women. Discharge from the primary hospital was faster after endovascular repair (hazard ratio 1.24, 95 per cent c.i. 1.04 to 1.47). For open repair, 30-day mortality diminished with increasing aneurysm neck length (adjusted odds ratio 0.69 (95 per cent c.i. 0.53 to 0.89) per 15 mm), but aortic diameter was not associated with mortality for either type of repair.
Conclusion: Survival to 90 days following an endovascular or open repair strategy is similar for all patients and for the restricted population anatomically suitable for endovascular repair. Women may benefit more from an endovascular strategy than men and patients are, on average, discharged sooner after endovascular repair.
© 2015 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
References
-
- Hinchliffe RJ, Bruijstens L, MacSweeney ST, Braithwaite BD. A randomised trial of endovascular and open surgery for ruptured abdominal aortic aneurysm – results of a pilot study and lessons learned for future studies. Eur J Vasc Endovasc Surg 2006; 32: 506–513. - PubMed
-
- Mastracci TM, Garrido‐Olivares L, Cinà CS, Clase CM. Endovascular repair of ruptured abdominal aortic aneurysms: a systematic review and meta‐analysis. J Vasc Surg 2008; 47: 214–221. - PubMed
-
- Harkin DW, Dillon M, Blair PH, Ellis PK, Kee F. Endovascular ruptured abdominal aortic aneurysm repair (EVRAR): a systematic review. Eur J Vasc Endovasc Surg 2007; 34: 673–681. - PubMed
-
- Reimerink JJ, Hoornweg LL, Vahl AC, Wisselink W, van den Broek TA, Legemate DA et al Endovascular repair versus open repair of ruptured abdominal aortic aneurysms: a multicenter randomized controlled trial. Ann Surg 2013; 258: 248–256. - PubMed
-
- Desgranges P, Kobeiter H, Katsahian S, Boufi M, Gouny P, Favre J‐P et al ECAR (Endovasculaire ou Chirurgie dans les Anévrysmes aorto‐iliaques Rompus): a French randomized controlled trial of endovascular vs. open surgical repair of ruptured aorto‐iliac aneurysms. Eur J Vasc Endovasc Surg 2015; [Epub ahead of print]. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
