

Productivity loss and indirect costs associated with cardiovascular events and related clinical procedures
- PMID: 26104784
- PMCID: PMC4478719
- DOI: 10.1186/s12913-015-0925-x
Productivity loss and indirect costs associated with cardiovascular events and related clinical procedures
Abstract
Background: The high acute costs of cardiovascular disease and acute cardiovascular events are well established, particularly in terms of direct medical costs. The costs associated with lost work productivity have been described in a broad sense, but little is known about workplace absenteeism or short term disability costs among high cardiovascular risk patients. The objective of this study was to quantify workplace absenteeism (WA) and short-term disability (STD) hours and costs associated with cardiovascular events and related clinical procedures (CVERP) in United States employees with high cardiovascular risk.
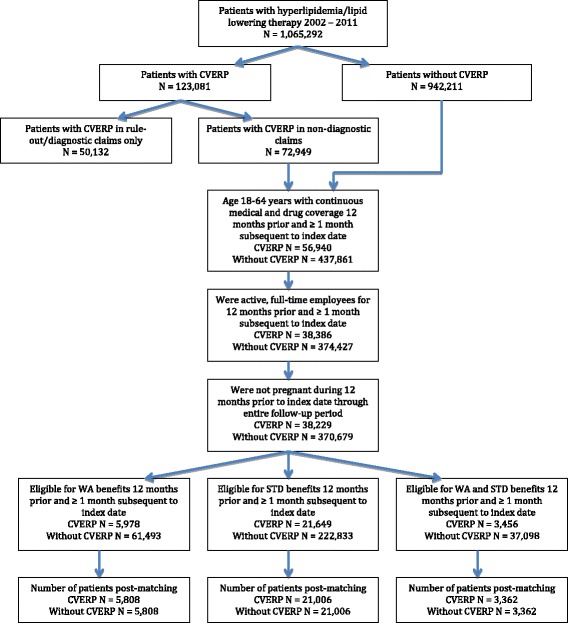
Methods: Medical, WA and/or STD data from the Truven Health MarketScan® Research Databases were used to select full-time employees aged 18-64 with hyperlipidemia during 2002-2011. Two cohorts (with and without CVERP) were created and screened for medical, drug, WA, and STD eligibility. The CVERP cohort was matched with a non-CVERP cohort using propensity score matching. Work loss hours and indirect costs were calculated for patients with and without CVERP and by CVERP type. Wages were based on the 2013 age-, gender-, and geographic region-adjusted wage rate from the United States Bureau of Labor Statistics.
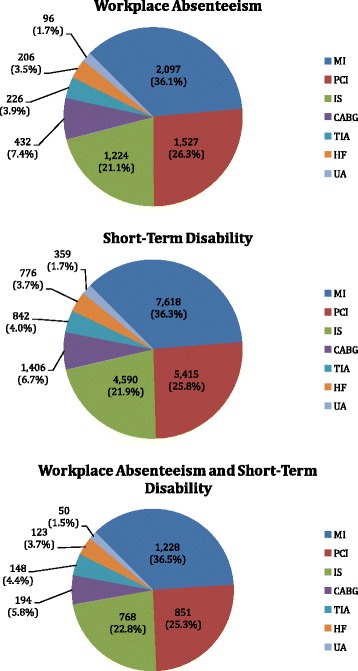
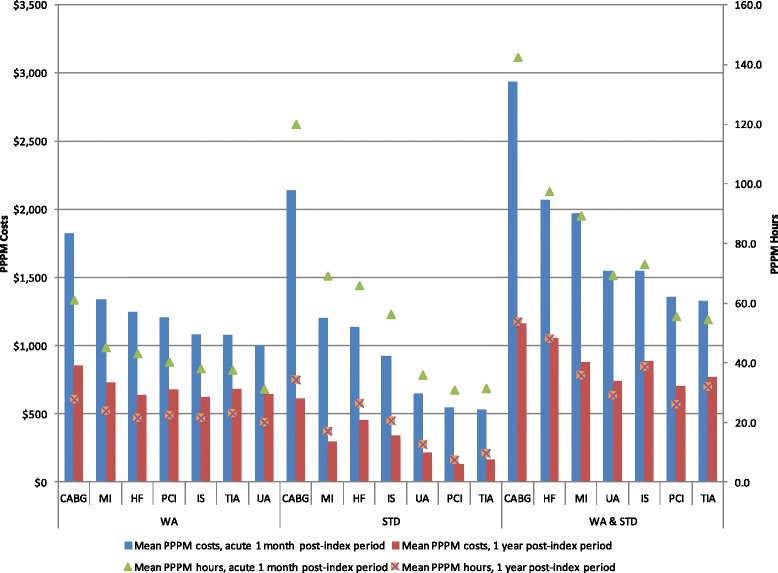
Results: A total of 5,808 WA-eligible, 21,006 STD-eligible, and 3,362 combined WA and STD eligible patients with CVERP were well matched to patients without CVERP, creating three cohorts of patients with CVERP and three cohorts of patients without CVERP. Demographics were similar across cohorts (mean age 52.2-53.1 years, male 81.3-86.8%). During the first month of follow-up, patients with CVERP had more WA/STD-related hours lost compared with patients without CVERP (WA-eligible: 23.4 more hours, STD-eligible: 51.7 more hours, WA and STD-eligible: 56.3 more hours) (p < 0.001). Corresponding costs were $683, $895, and $1,119 higher, respectively (p < 0.001). Differences narrowed with longer follow-up. In the first month and year of follow-up, patients with coronary artery bypass graft experienced the highest WA/STD-related hours lost and costs compared with patients with other CVERP.
Conclusions: CVERP were associated with substantial work loss and indirect costs. Prevention or reduction of CVERP could result in WA and STD-related cost savings for employers.
Figures
References
-
- Waters DD, Brotons C, Chiang CW, Ferrieres J, Foody J, Jukema JW, et al. Lipid treatment assessment project 2: a multinational survey to evaluate the proportion of patients achieving low-density lipoprotein cholesterol goals. Circulation. 2009;120:28–34. doi: 10.1161/CIRCULATIONAHA.108.838466. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
