

Prevalence and prognostic impact of chronic kidney disease in STEMI from a gender perspective: data from the SWEDEHEART register, a large Swedish prospective cohort
- PMID: 26105033
- PMCID: PMC4480024
- DOI: 10.1136/bmjopen-2015-008188
Prevalence and prognostic impact of chronic kidney disease in STEMI from a gender perspective: data from the SWEDEHEART register, a large Swedish prospective cohort
Abstract
Objectives: Gender differences in prevalence and prognostic impact of chronic kidney disease (CKD) in ST segment elevation myocardial infarction (STEMI) have been poorly evaluated. In STEMI, female gender has been independently associated with an increased risk of mortality. CKD has been found to be an important prognostic marker in myocardial infarction. The aim of this study was to evaluate gender differences in prevalence and prognostic impact of CKD on short-term and long-term mortality.
Design: Prospective observational cohort study.
Setting: The national quality register SWEDEHEART was used. In the beginning of the study period, 94% of the Swedish coronary care units contributed data to the register, which subsequently increased to 100%. The glomerular filtration rate was estimated (eGFR) according to Modification of Diet in Renal Disease Study (MDRD) and Cockcroft-Gault (CG).
Participants: All patients with STEMI registered in SWEDEHEART from the years 2003-2009 were included (37,991 patients, 66% men).
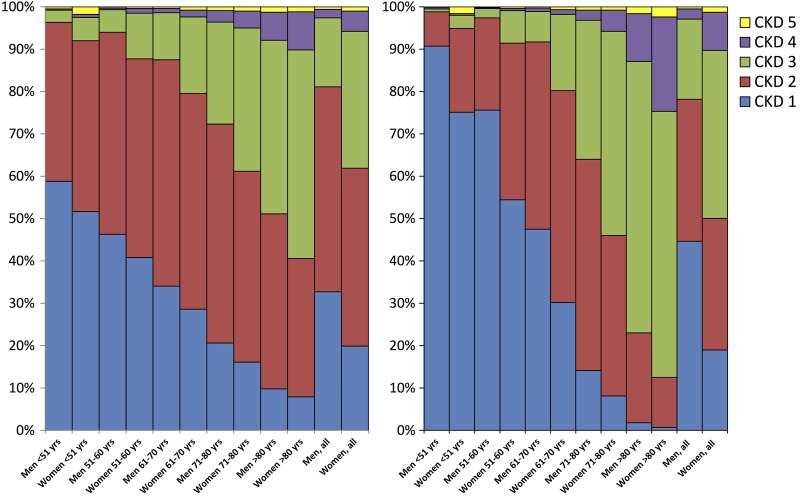
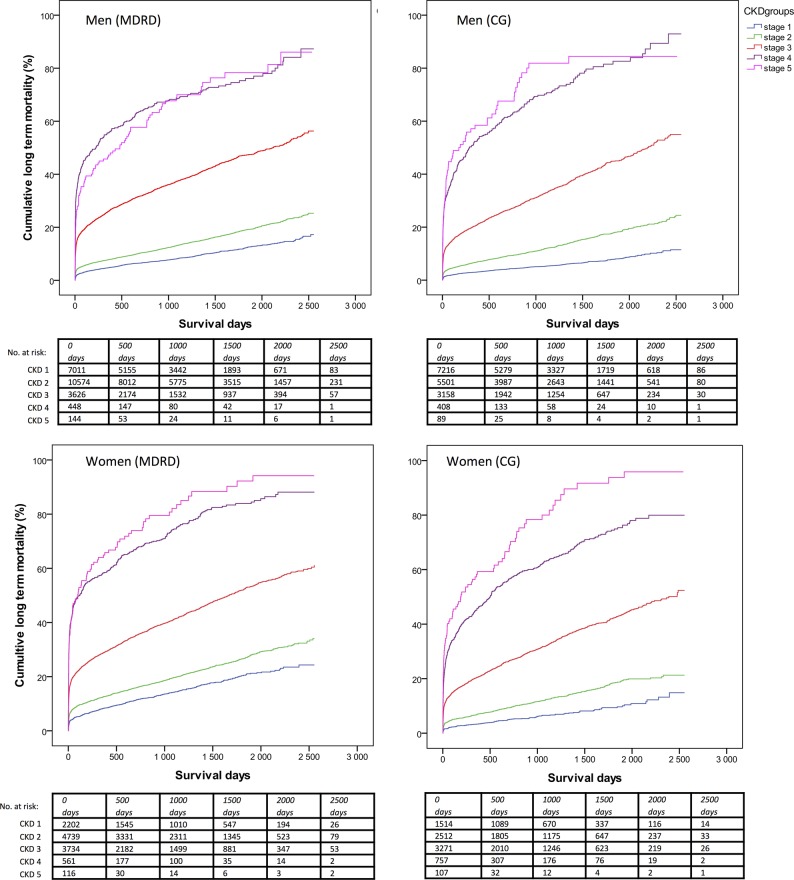
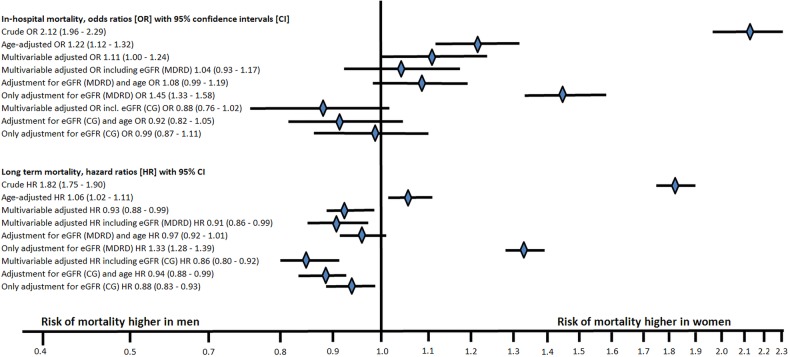
Main results: Women had 1.6 (MDRD) to 2.2 (CG) times higher multivariable adjusted risk of CKD. Half of the women had CKD according to CG. CKD was associated with 2-2.5 times higher risk of in-hospital mortality and approximately 1.5 times higher risk of long-term mortality in both genders. Each 10 mL/min decline of eGFR was associated with an increased risk of in-hospital and long-term mortality (22-33% and 9-16%, respectively) and this did not vary significantly by gender. Both in-hospital and long-term mortality were doubled in women. After multivariable adjustment including eGFR, there was no longer any gender difference in early outcome and the long-term outcome was better in women.
Conclusions: Among patients with STEMI, female gender was independently associated with CKD. Reduced eGFR was a strong independent risk factor for short-term and long-term mortality without a significant gender difference in prognostic impact and seems to be an important reason why women have higher mortality than men with STEMI.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- Gibson CM, Dumaine RL, Gelfand EV et al. . Association of glomerular filtration rate on presentation with subsequent mortality in non-ST-segment elevation acute coronary syndrome; observations in 13,307 patients in five TIMI trials. Eur Heart J 2004;25:1998–2005. 10.1016/j.ehj.2004.08.016 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous