

doi: 10.1155/2015/354158.
Epub 2015 May 27.
Synchronous Multicentric Giant Cell Tumour of Distal Radius and Sacrum with Pulmonary Metastases
Affiliations
- PMID: 26106496
- PMCID: PMC4461722
- DOI: 10.1155/2015/354158
Item in Clipboard
Synchronous Multicentric Giant Cell Tumour of Distal Radius and Sacrum with Pulmonary Metastases
Case Rep Oncol Med.
2015.
Abstract
Giant cell tumour (GCT) is an uncommon primary bone tumour, and its multicentric presentation is exceedingly rare. We report a case of a 45-year-old female who presented to us with GCT of left distal radius. On the skeletal survey, osteolytic lesion was noted in her right sacral ala. Biopsy confirmed both lesions as GCT. Pulmonary metastasis was also present. Resection-reconstruction arthroplasty for distal radius and thorough curettage and bone grafting of the sacral lesion were done. Multicentric GCT involving distal radius and sacrum with primary sacral involvement is not reported so far to our knowledge.
Figures

(a and b) Preop plain radiograph of left wrist showing expansile solitary lytic lesion involving left distal radius; (c and d) postoperative radiographs after resection and reconstruction arthroplasty of left wrist; (e) radiographs of her left wrist showing wrist subluxation following k-wire removal; (f) 1 year follow-up radiograph of her left wrist with gross subluxation of wrist.
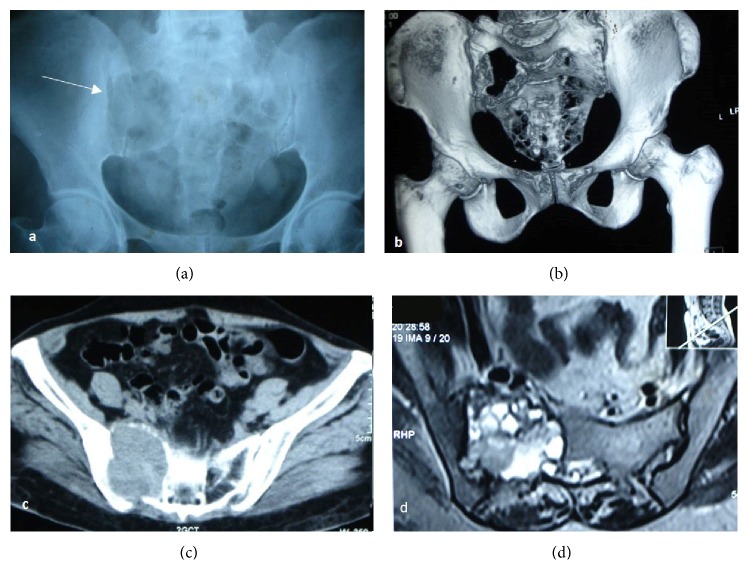
(a) Radiograph of the pelvis AP view; (b) 3D reconstruction and (c) axial section of CT showing expansile lytic lesion involving the right sacral ala with cortical break and surrounding soft-tissue component extending into right SI joint space and pelvis measuring 5.2 × 5.7 × 6.3 cm eroding the adjacent iliac bone. Mass extending into the sacral canal. (d) MRI showing large expansile heterogeneous lobulated lesion with few septations involving right sacroiliac joint. Predominantly lytic lesion with cortical destruction features suggestive of GCT.
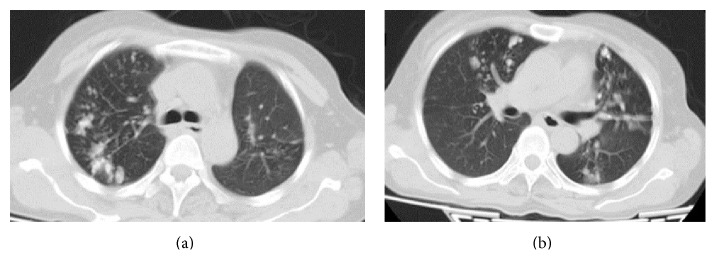
Multiple irregular opacities in apical segments of right upper lobe and left lingular superior segment, anterobasal and posterobasal segments suggestive of metastasis.
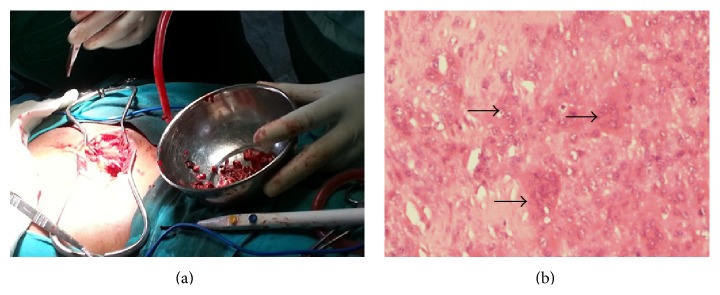
(a) Intraoperative photograph of curettage and bone grafting of the sacral lesion; (b) histopathology slide showing characteristic osteoclast like giant cells (arrows) in the background of mononuclear cells.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
