

Cerebellar infarct patterns: The SMART-Medea study
- PMID: 26106556
- PMCID: PMC4473120
- DOI: 10.1016/j.nicl.2015.02.001
Cerebellar infarct patterns: The SMART-Medea study
Abstract
Objective: Previous studies on cerebellar infarcts have been largely restricted to acute infarcts in patients with clinical symptoms, and cerebellar infarcts have been evaluated with the almost exclusive use of transversal MR images. We aimed to document the occurrence and 3D-imaging patterns of cerebellar infarcts presenting as an incidental finding on MRI.
Methods: We analysed the 1.5 Tesla MRI, including 3D T1-weighted datasets, of 636 patients (mean age 62 ± 9 years, 81% male) from the SMART-Medea study. Cerebellar infarct analyses included an assessment of size, cavitation and gliosis, of grey and white matter involvement, and of infarct topography.
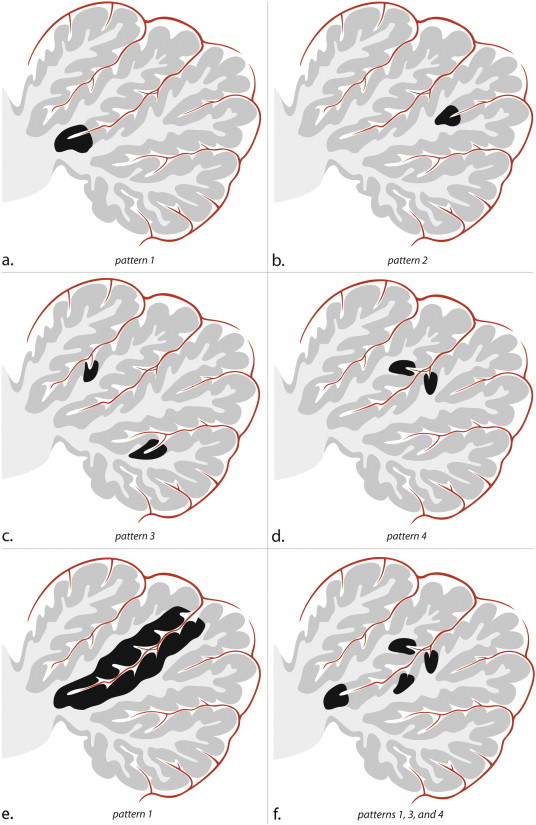
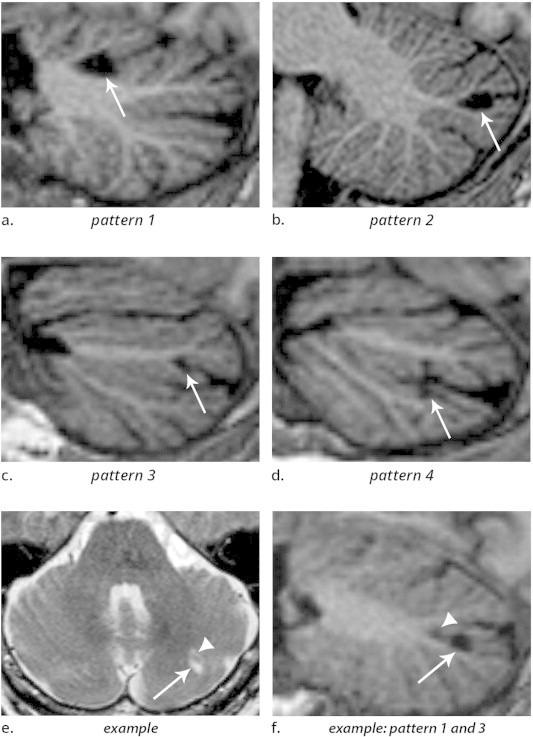
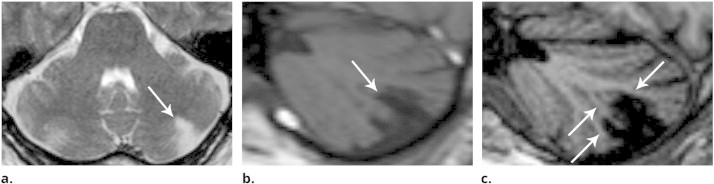
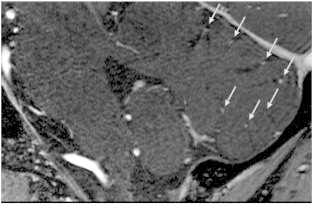
Results: One or more cerebellar infarcts (mean 1.97; range 1-11) were detected in 70 out of 636 patients (11%), with a total amount of 138 infarcts identified, 135 of which showed evidence of cavitation. The average mean axial diameter was 7 mm (range 2-54 mm), and 131 infarcts (95%) were smaller than 20 mm. Hundred-thirty-four infarcts (97%) involved the cortex, of which 12 in combination with subcortical white matter. No infarcts were restricted to subcortical branches of white matter. Small cortical infarcts involved the apex of a deep (pattern 1) or shallow fissure (pattern 2), or occurred alongside one (pattern 3) or opposite sides (pattern 4) of a fissure. Most (87%) cerebellar infarcts were situated in the posterior lobe.
Conclusions: Small cerebellar infarcts proved to be much more common than larger infarcts, and preferentially involved the cortex. Small cortical infarcts predominantly involved the posterior lobes, showed sparing of subcortical white matter and occurred in characteristic topographic patterns.
Keywords: Cerebellum; Cerebrovascular disease; MRI.
Figures
References
-
- Bogousslavsky J., Regli F., Maeder P. The etiology of posterior circulation infarcts: a prospective study using magnetic resonance imaging and magnetic resonance angiography. Neurol. 1993;43(8):1528–1533. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
