

Rotation-invariant multi-contrast non-local means for MS lesion segmentation
- PMID: 26106563
- PMCID: PMC4474283
- DOI: 10.1016/j.nicl.2015.05.001
Rotation-invariant multi-contrast non-local means for MS lesion segmentation
Abstract
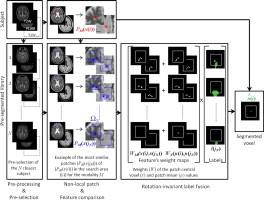
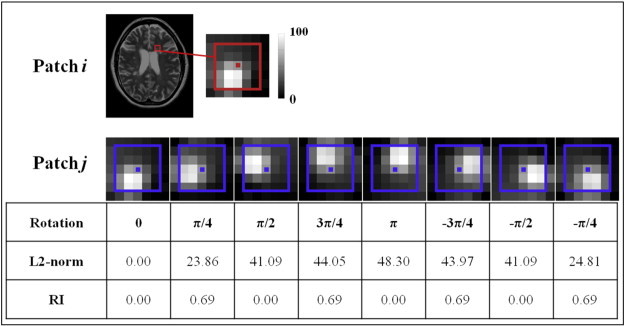
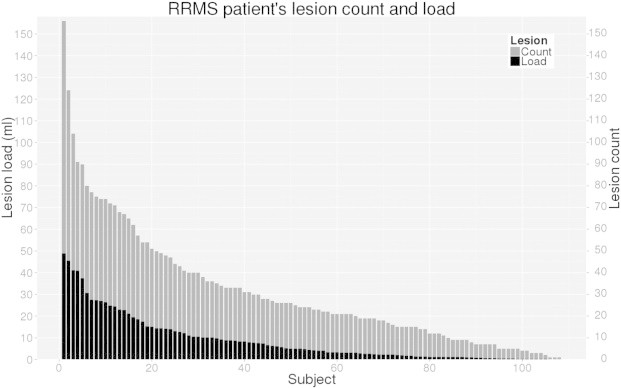
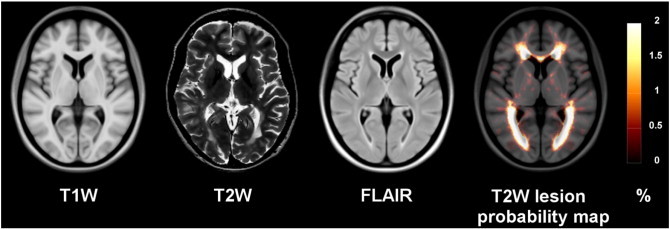
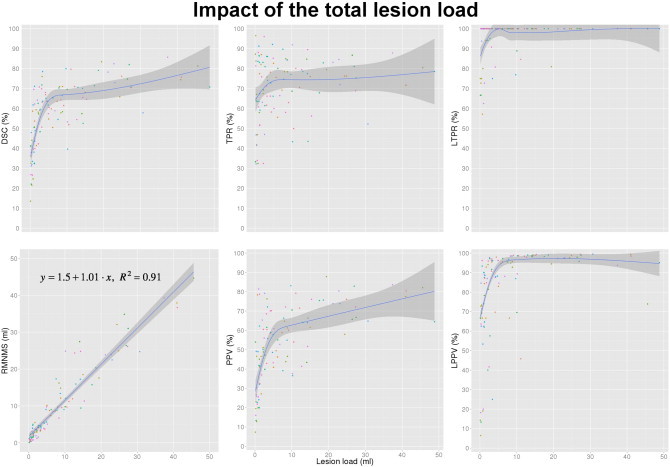
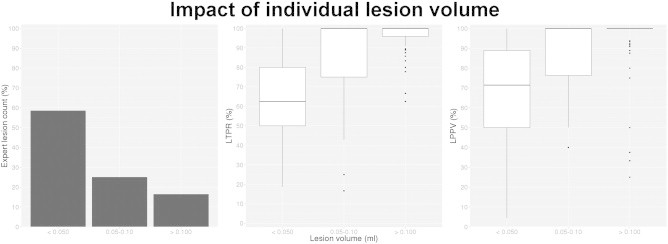
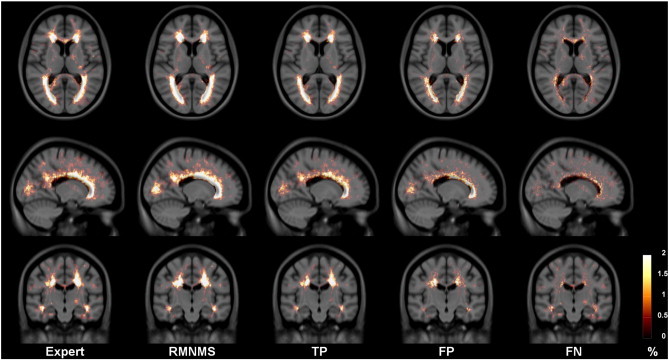
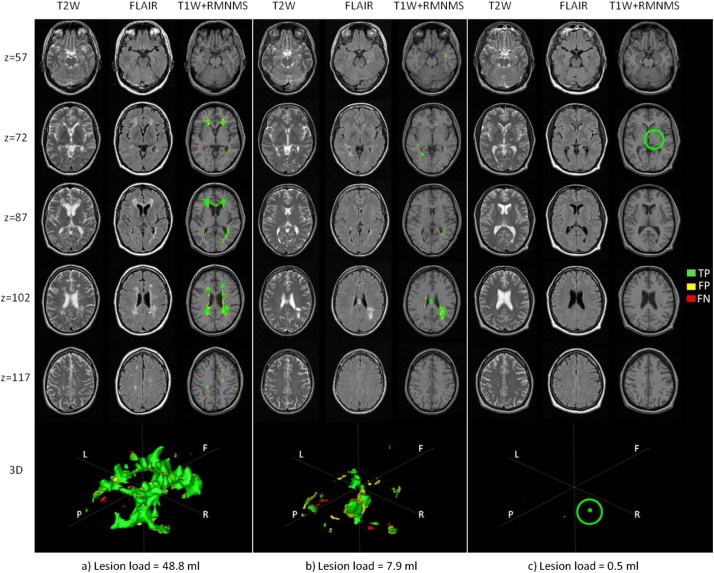
Multiple sclerosis (MS) lesion segmentation is crucial for evaluating disease burden, determining disease progression and measuring the impact of new clinical treatments. MS lesions can vary in size, location and intensity, making automatic segmentation challenging. In this paper, we propose a new supervised method to segment MS lesions from 3D magnetic resonance (MR) images using non-local means (NLM). The method uses a multi-channel and rotation-invariant distance measure to account for the diversity of MS lesions. The proposed segmentation method, rotation-invariant multi-contrast non-local means segmentation (RMNMS), captures the MS lesion spatial distribution and can accurately and robustly identify lesions regardless of their orientation, shape or size. An internal validation on a large clinical magnetic resonance imaging (MRI) dataset of MS patients demonstrated a good similarity measure result (Dice similarity = 60.1% and sensitivity = 75.4%), a strong correlation between expert and automatic lesion load volumes (R(2) = 0.91), and a strong ability to detect lesions of different sizes and in varying spatial locations (lesion detection rate = 79.8%). On the independent MS Grand Challenge (MSGC) dataset validation, our method provided competitive results with state-of-the-art supervised and unsupervised methods. Qualitative visual and quantitative voxel- and lesion-wise evaluations demonstrated the accuracy of RMNMS method.
Keywords: MRI; MS lesions; MSGC; Multi-contrast; Non-local; Patch-based; Segmentation; Supervised.
Figures
References
-
- Bai W., Shi W., O'Regan D.P., Tong T., Wang H., Jamil-Copley S., Peters N.S., Rueckert D. A probabilistic patch-based label fusion model for multi-atlas segmentation with registration refinement: application to cardiac MR images. I.E.E.E. Transactions Med. Imaging. 2013;32(7):1302–1315. 23568495 - PubMed
-
- Borgefors G. Hierarchical chamfer matching: a parametric edge matching algorithm. IEEE Trans. Pattern Anal. Machine Intell. 1988;10(6):849–865.
-
- Buades A., Coll B., Morel J.M. CVPR 2005. I.E.E.E. Computer Society Conference. IEEE; 2005. A non-local algorithm for image denoising. Computer vision and pattern recognition.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
