

Model for End-Stage Liver Disease, Model for Liver Transplantation Survival and Donor Risk Index as predictive models of survival after liver transplantation in 1,006 patients
- PMID: 26106959
- PMCID: PMC4462569
- DOI: 10.6061/clinics/2015(06)05
Model for End-Stage Liver Disease, Model for Liver Transplantation Survival and Donor Risk Index as predictive models of survival after liver transplantation in 1,006 patients
Abstract
Objectives: Liver transplantation has not increased with the number of patients requiring this treatment, increasing deaths among those on the waiting list. Models predicting post-transplantation survival, including the Model for Liver Transplantation Survival and the Donor Risk Index, have been created. Our aim was to compare the performance of the Model for End-Stage Liver Disease, the Model for Liver Transplantation Survival and the Donor Risk Index as prognostic models for survival after liver transplantation.
Method: We retrospectively analyzed the data from 1,270 patients who received a liver transplant from a deceased donor in the state of São Paulo, Brazil, between July 2006 and July 2009. All data obtained from the Health Department of the State of São Paulo at the 15 registered transplant centers were analyzed. Patients younger than 13 years of age or with acute liver failure were excluded.
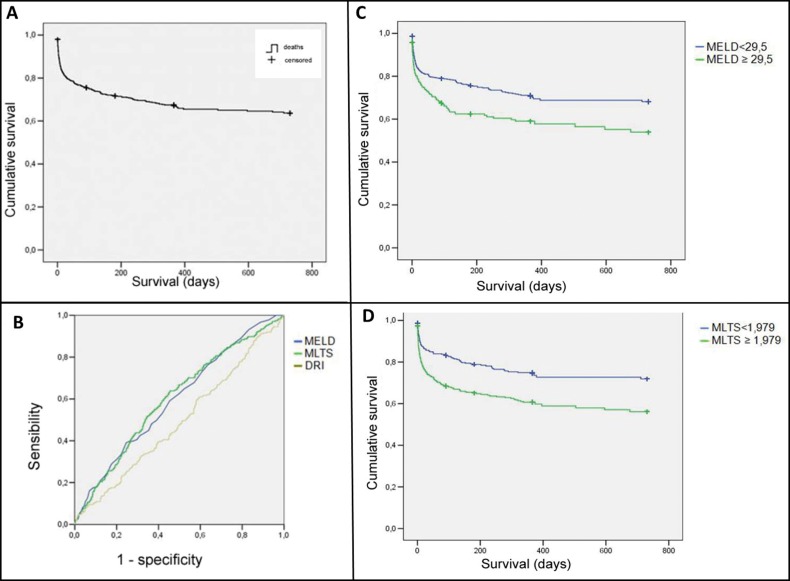
Results: The majority of the recipients had Child-Pugh class B or C cirrhosis (63.5%). Among the 1,006 patients included, 274 (27%) died. Univariate survival analysis using a Cox proportional hazards model showed hazard ratios of 1.02 and 1.43 for the Model for End-Stage Liver Disease and the Model for Liver Transplantation Survival, respectively (p<0.001). The areas under the ROC curve for the Donor Risk Index were always less than 0.5, whereas those for the Model for End-Stage Liver Disease and the Model for Liver Transplantation Survival were significantly greater than 0.5 (p<0.001). The cutoff values for the Model for End-Stage Liver Disease (≥29.5; sensitivity: 39.1%; specificity: 75.4%) and the Model for Liver Transplantation Survival (≥1.9; sensitivity 63.9%, specificity 54.5%), which were calculated using data available before liver transplantation, were good predictors of survival after liver transplantation (p<0.001).
Conclusions: The Model for Liver Transplantation Survival displayed similar death prediction performance to that of the Model for End-Stage Liver Disease. A simpler model involving fewer variables, such as the Model for End-Stage Liver Disease, is preferred over a complex model involving more variables, such as the Model for Liver Transplantation Survival. The Donor Risk Index had no significance in post-transplantation survival in our patients.
Conflict of interest statement
No potential conflict of interest was reported.
Figures
References
-
- Eagle KA. Surgical patients with heart disease: summary of the ACC/AHA guidelines. American College of Cardiology/American Heart Association. Am Fam Physician. 1997;56((3)):811–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
