

A propose of pulmonary dysfunction stratification after valve surgery by physiotherapeutic assistance level
- PMID: 26107450
- PMCID: PMC4462964
- DOI: 10.5935/1678-9741.20150006
A propose of pulmonary dysfunction stratification after valve surgery by physiotherapeutic assistance level
Abstract
Objective: a) to propose and implement an evaluation system; b) to classify the pulmonary involvement and determine levels of physical therapy; c) to check the progress postoperatively.
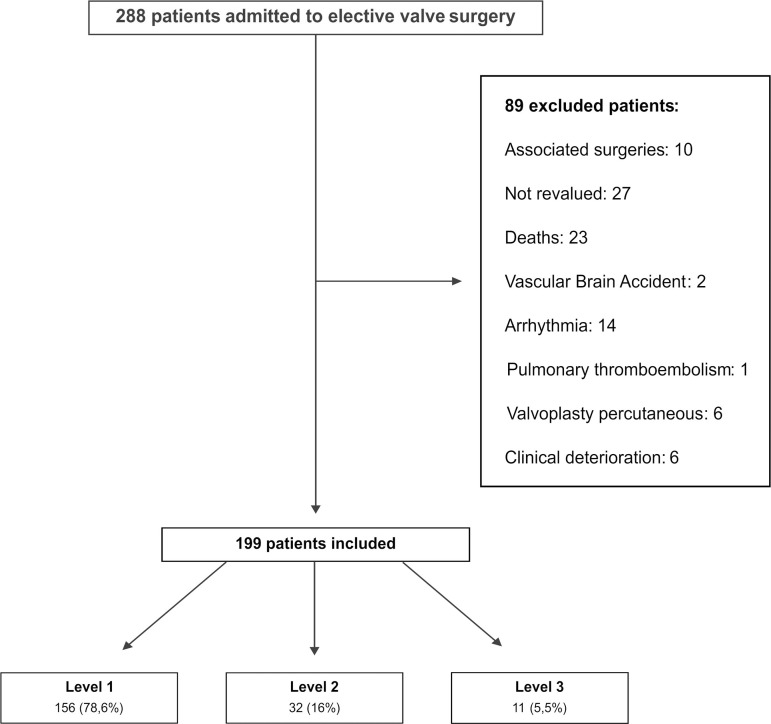
Methods: Patients underwent physiotherapy assessment preoperatively, postoperatively and after 5 days of intervention. They were classified into three levels of care: level 1 - low risk of complication; Level 2 - medium risk; Level 3 - high risk. We used analysis of variance and Kruskal-Wallis and analysis of variance for repeated measures or Friedman. Chi-square test or Fisher for proportions. We considered statistical significance level P<0.05.
Results: We studied 199 patients, 156 classified within level 1, 32 at level 2 and 11 at level 3. Thoracoabdominal motion and auscultation changed significantly postoperatively, persisting at levels 2 and 3 (P<0.05). Oxygenation and respiratory rate changed at levels 2 and 3 postoperatively (P<0.05) with recovery at the end. Significant decrease in lung volumes occurred in three levels (P<0.05) with partial recovery at level 1, lung collapse occurred at all levels, with recovery by 56% at level 1, 47% at level 2, 27% at level 3.
Conclusion: The proposed assessment identified valve surgery patients who require differentiated physical therapy. Level 1 patients had rapid recovery, while the level 2 showed significant changes with functional gains at the end. Level 3 patients, more committed and prolonged recovery, should receive greater assistance.
Objetivo: a) propor e aplicar um sistema de avaliação; b) classificar o comprometimento pulmonar e determinar os níveis de assistência fisioterapêutica; c) verificar a evolução no pós-operatório de cirurgia valvar.
Métodos: Pacientes realizaram avaliação fisioterapêutica no pré-operatório, pós-operatório e após 5 dias de intervenção. Foram classificados em três níveis de atenção: nível 1 - baixo risco de complicação; nível 2 - médio risco; nível 3 - alto risco. Utilizou-se Análise de Variância e Kruskal-Wallis e Análise de Variância para medidas repetidas ou Friedmann. Teste qui-quadrado ou Fisher para as proporções. Considerou-se nível de significância estatística P<0,05.
Resultados: Foram estudados 199 pacientes, 156 classificados no nível 1, 32 nível 2 e 11 nível 3. Movimento toracoabdominal e ausculta pulmonar alteraram significantemente no pós-operatório, persistindo nos níveis 2 e 3 (P<0,05). Oxigenação e frequência respiratória se modificaram nos níveis 2 e 3 no pós-operatório (P<0,05), com recuperação no final. Diminuição significante dos volumes pulmonares ocorreu nos três níveis (P<0,05), com recuperação parcial no nível 1. Colapso pulmonar ocorreu em todos os níveis, com recuperação em 56% no nível 1, 47% no nível 2, 27% no nível 3.
Conclusão: A avaliação proposta identificou pacientes de cirurgia valvar que necessitam de assistência fisioterapêutica diferenciada. Pacientes do nível 1 tiveram rápida recuperação, enquanto os do nível 2 mostraram alterações significativas, com ganhos funcionais no final. Pacientes do nível 3, mais comprometidos e com recuperação prolongada, devem receber maior assistência.
Conflict of interest statement
Potential Conflict of Interest The authors declare no conflict of interest.
Figures



References
-
- Sia S, D'Andrea V, Mamone D, Pagnotta L, Verre M. Early postoperative hypoxemia: incidence and effectiveness of oxygen administration. Minerva Anestesiol. 1994;60(11):657–662. - PubMed
-
- Szeles TF, Yoshinaga EM, Alenca W, Brudniewski M, Ferreira FS, Auler JO, et al. Hypoxemia after myocardial revascularization: analysis of risk factors. Rev Bras Anestesiol. 2008;58(2):124–136. - PubMed
-
- Taggart DP, El-Fiky M, Carter R, Bowman A, Wheatley DJ. Respiratory dysfunction after uncomplicated cardiopulmonary bypass. Ann Thorac Surg. 1993;56(5):1123–1128. - PubMed
-
- Matthay MA, Wiener Kronish JP. Respiratory management after cardiac surgery. Chest. 1989;95(2):424–434. - PubMed
-
- Singh NP, Vargas FS, Cukier A, Terra-Filho M, Teixeira LR, Light RW. Arterial blood gases after coronary artery bypass surgery. Chest. 1992;102(5):1337–1341. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical