

Surgical treatment of complex aneurysms and thoracic aortic dissections with the Frozen Elephant Trunk technique
- PMID: 26107452
- PMCID: PMC4462966
- DOI: 10.5935/1678-9741.20140119
Surgical treatment of complex aneurysms and thoracic aortic dissections with the Frozen Elephant Trunk technique
Abstract
Objective: Report initial experience with the Frozen Elephant Trunk technique.
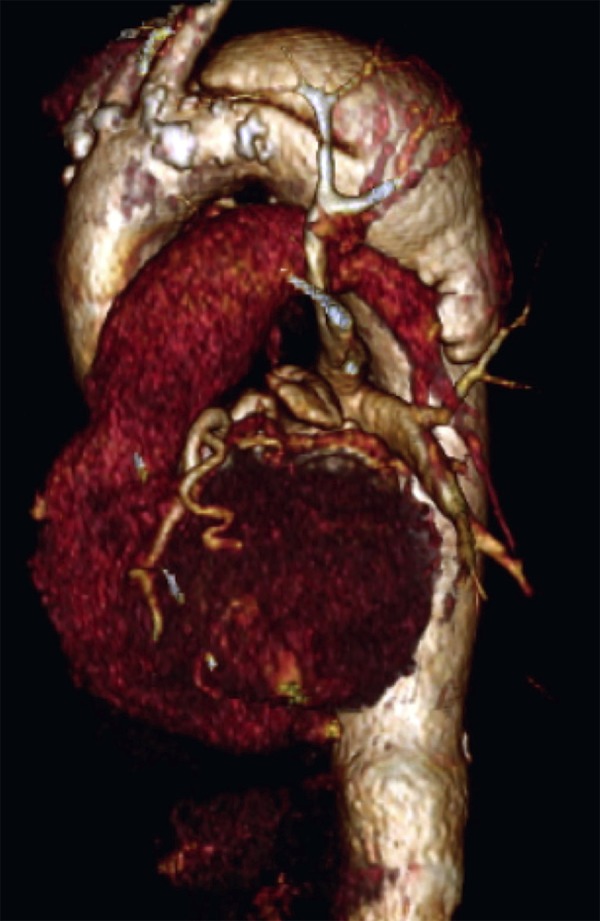
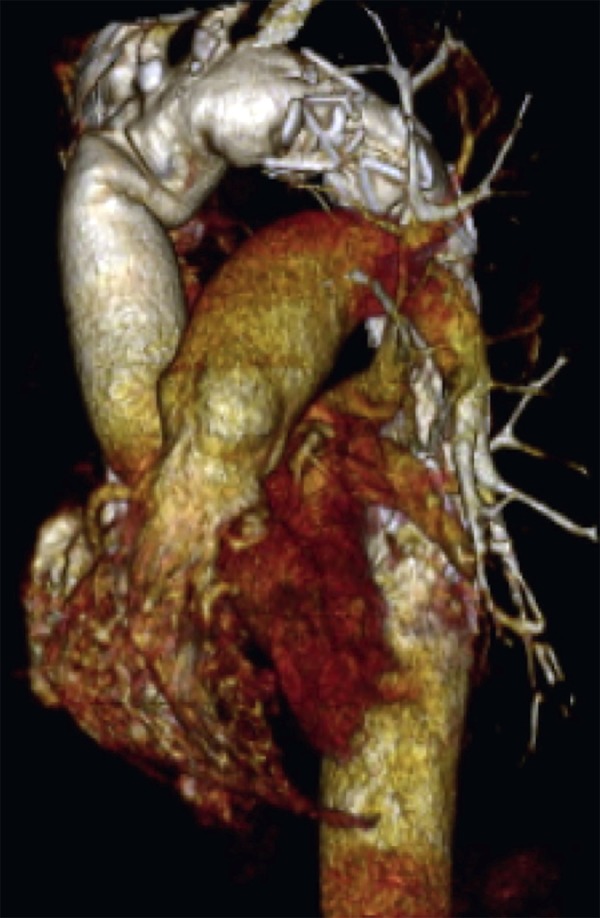
Methods: From July 2009 to October 2013, Frozen Elephant Trunk technique was performed in 21 patients (66% male, mean age 56 ± 11 years). They had type A aortic dissection (acute 9.6%, chronic 57.3%), type B (14.3%, all chronic) and complex aneurysms (19%). It was 9.5% of reoperations and 38% of associated procedures (25.3% miocardial revascularization, 25.3% replacement of aortic valve and 49.4% aortic valved graft). Aortic remodeling was evaluated comparing preoperative and most recent computed tomography scans. One hundred per cent of complete follow-up, mean time of 28 months.
Results: In-hospital mortality of 14.2%, being 50% in acute type A aortic dissection, 8.3% in chronic type A aortic dissection, 33.3% in chronic type B aortic dissection and 0% in complex aneurysms. Mean times of cardiopulmonary bypass (152 ± 24 min), myocardial ischemia (115 ± 31 min) and selective cerebral perfusion (60 ± 15 min). Main complications were bleeding (14.2%), spinal cord injury (9.5%), stroke (4.7%), prolonged mechanical ventilation (4.7%) and acute renal failure (4.7%). The need for second-stage operation was 19%. False-lumen thrombosis was obtained in 80%.
Conclusion: Frozen Elephant Trunk is a feasible technique and should be considered. The severity of the underlying disease justifies high mortality rates. The learning curve is a reality. This approach allows treatment of more than two segments at once. Nonetheless, if a second stage is made necessary, it is facilitated.
Objetivo: Relatar experiência inicial com a técnica "Frozen Elephant Trunk".
Métodos: Entre julho de 2009 e outubro de 2013, 21 pacientes, 66% homens, média de idade de 56±11 anos, 66,7% portadores de dissecção da aorta tipo A de Stanford (9,6% agudas e 57,1% crônicas), tipo B (14,3%, todas crônicas) e aneurismas complexos (19%), foram operados pela técnica Frozen Elephant Trunk. Foram 9,5% de reoperações e 38% com procedimentos associados (25,3% revascularizações do miocárdio, 25,3% troca da valva aórtica e 49,4% tubos valvulados). Remodelamento da aorta foi avaliado com a comparação de angiotomografia pré-operatória e pós-operatória mais recente. Seguimento 100% dos pacientes, tempo médio de 28 meses.
Resultados: Mortalidade hospitalar de 14,2%, sendo 50% nas dissecções do tipo A agudas, 8,3% nas tipo A crônicas, 33,3% nas tipo B crônicas e 0% nos aneurismas complexos. Tempos médios de CEC (152±24min), isquemia miocárdica (115±31min) e perfusão cerebral seletiva (60±15min). Principais complicações pós-operatórias foram sangramento (14,2%), acidente vascular encefálico (4,7%), paraplegia (9,5%), intubação>72h (4,7%) e insuficiência renal aguda (4,7%). Houve necessidade de complementação do tratamento (distal ao stent) em 19%. Houve trombose da falsa luz em 80%.
Conclusão: Frozen Elephant Trunk é opção técnica a ser utilizada. A gravidade e extensão da doença justificam mortalidade mais elevada. A curva de aprendizado é uma realidade. Esta abordagem permite abordar mais de dois segmentos de aorta em um estágio, mas se necessário segundo estágio, este é facilitado.
Figures
Comment in
-
Key points of reducing neurologic complications in frozen elephant trunk technique.Rev Bras Cir Cardiovasc. 2015 Jul-Aug;30(4):505-6. doi: 10.5935/1678-9741.20150056. Rev Bras Cir Cardiovasc. 2015. PMID: 27163429 Free PMC article. No abstract available.
-
Answer to "Key points of reducing neurologic complications in frozen elephant trunk technique".Rev Bras Cir Cardiovasc. 2015 Jul-Aug;30(4):506. doi: 10.5935/1678-9741.20150057. Rev Bras Cir Cardiovasc. 2015. PMID: 27163430 Free PMC article. No abstract available.
References
-
- Kato M, Ohnishi K, Kaneko M, Ueda T, Kishi D, Mizushima T, et al. New graft-implanting method for thoracic aortic aneurysm or dissection with a stented graft. Circulation. 1996;94(9) Suppl I:II188–II193. - PubMed
-
- Borst HG, Walterbusch G, Schaps D. Extensive aortic replacement using 'elephant trunk' prosthesis. Thorac Cardiovasc Surg. 1983;31(1):37–40. - PubMed
-
- Halstead JC, Meier M, Etz C, Spielvogel D, Bodian C, Wurm M, et al. The fate of the distal aorta after repair of acute type A aortic dissection. J Thorac Cardiovasc Surg. 2007;133(1):127–135. - PubMed
-
- Song SW, Chang BC, Cho BK, Yi G, Youn YN, Lee S, et al. Effects of partial thrombosis on distal aorta after repair of acute DeBakey type I aortic dissection. J Thorac Cardiovasc Surg. 2010;139(4):841–847. - PubMed
-
- Kim JB, Lee CH, Lee TY, Jung SH, Choo SJ, Lee JW, et al. Descending aortic aneurysmal changes following surgery for acute DeBakey type I aortic dissection. Eur J Cardiothorac Surg. 2012;42(5):851–856. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources