

Modeling the Health and Economic Burden of Hepatitis C Virus in Switzerland
- PMID: 26107467
- PMCID: PMC4480969
- DOI: 10.1371/journal.pone.0125214
Modeling the Health and Economic Burden of Hepatitis C Virus in Switzerland
Abstract
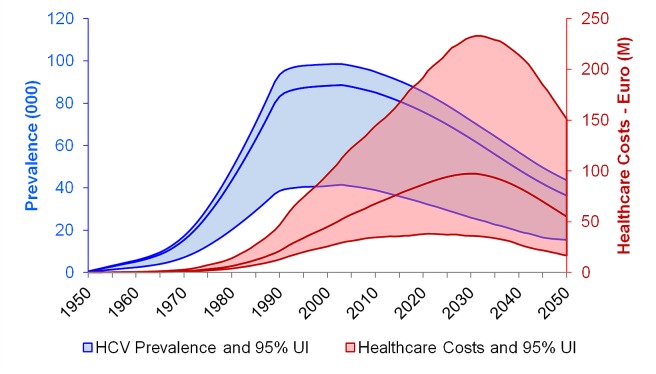
Background: Chronic hepatitis C virus infection is a major cause of liver disease in Switzerland and carries a significant cost burden. Currently, only conservative strategies are in place to mitigate the burden of hepatitis C in Switzerland. This study expands on previously described modeling efforts to explore the impact of: no treatment, and treatment to reduce HCC and mortality. Furthermore, the costs associated with untreated HCV were modeled.
Methods: Hepatitis C disease progression and mortality were modeled. Baseline historical assumptions were collected from the literature and expert interviews and strategies were developed to show the impact of different levels of intervention (improved drug cure rates, treatment and diagnosis) until 2030.
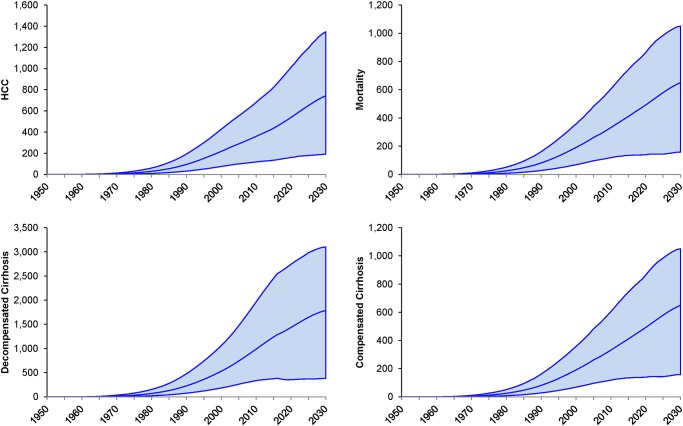
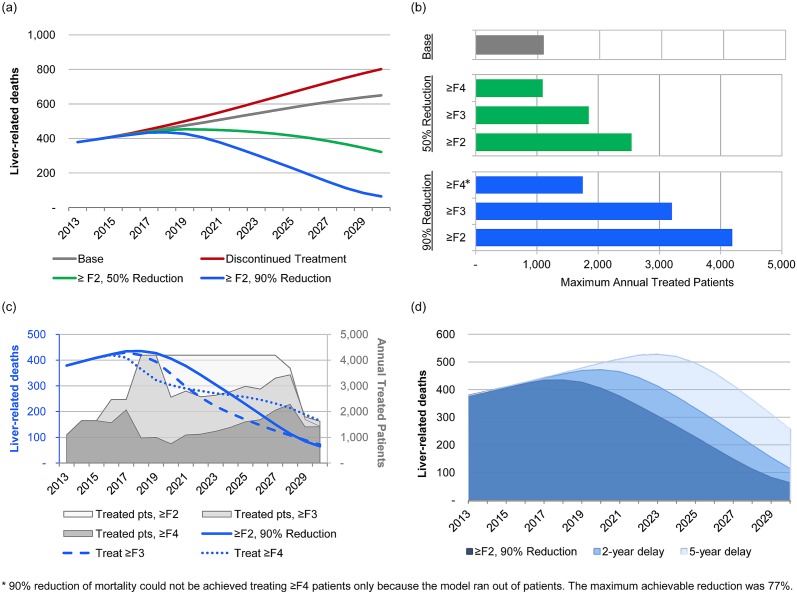
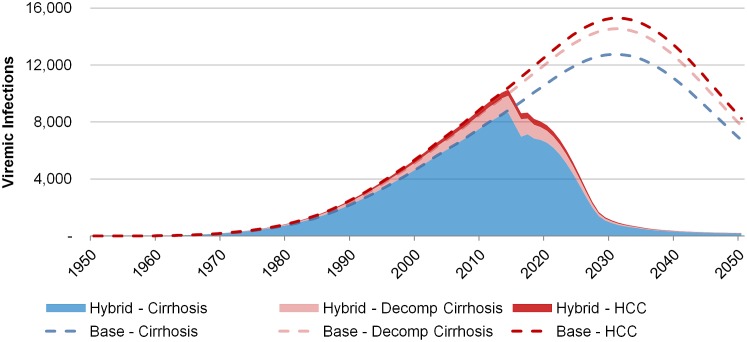
Results: Under the historical standard of care, the number of advanced stage cases was projected to increase until 2030, at which point the annual economic burden of untreated viremic infections was projected to reach €96.8 (95% Uncertainty Interval: €36 - €232) million. Scenarios to reduce HCV liver-related mortality by 90% by 2030 required treatment of 4,190 ≥F2 or 3,200 ≥F3 patients annually by 2018 using antivirals with a 95% efficacy rate. Delaying the implementation of these scenarios by 2 or 5 years reduced the impact on mortality to 75% and 57%, respectively.
Conclusions: With today's treatment efficacy and uptake rates, hepatitis C disease burden is expected to increase through 2030. A substantial reduction in disease burden can be achieved by means of both higher efficacy drugs and increased treatment uptake. However, these efforts cannot be undertaken without a simultaneous effort to diagnose more infections.
Conflict of interest statement
Figures
References
-
- World Health Organization—Department of Immunization VaB (2006) State of the art of new vaccine research and development. Geneva, Switzerland: WHO/IVB/06.01: 1–112.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
