

Effects of diabetes definition on global surveillance of diabetes prevalence and diagnosis: a pooled analysis of 96 population-based studies with 331,288 participants
- PMID: 26109024
- PMCID: PMC4673089
- DOI: 10.1016/S2213-8587(15)00129-1
Effects of diabetes definition on global surveillance of diabetes prevalence and diagnosis: a pooled analysis of 96 population-based studies with 331,288 participants
Abstract
Background: Diabetes has been defined on the basis of different biomarkers, including fasting plasma glucose (FPG), 2-h plasma glucose in an oral glucose tolerance test (2hOGTT), and HbA1c. We assessed the effect of different diagnostic definitions on both the population prevalence of diabetes and the classification of previously undiagnosed individuals as having diabetes versus not having diabetes in a pooled analysis of data from population-based health examination surveys in different regions.
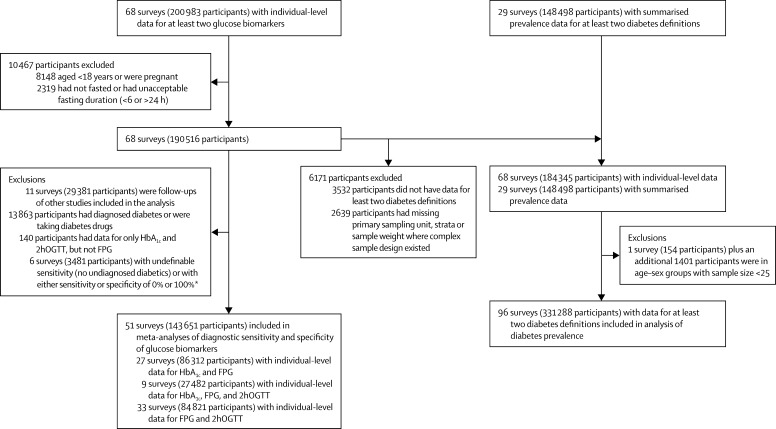
Methods: We used data from 96 population-based health examination surveys that had measured at least two of the biomarkers used for defining diabetes. Diabetes was defined using HbA1c (HbA1c ≥6·5% or history of diabetes diagnosis or using insulin or oral hypoglycaemic drugs) compared with either FPG only or FPG-or-2hOGTT definitions (FPG ≥7·0 mmol/L or 2hOGTT ≥11·1 mmol/L or history of diabetes or using insulin or oral hypoglycaemic drugs). We calculated diabetes prevalence, taking into account complex survey design and survey sample weights. We compared the prevalences of diabetes using different definitions graphically and by regression analyses. We calculated sensitivity and specificity of diabetes diagnosis based on HbA1c compared with diagnosis based on glucose among previously undiagnosed individuals (ie, excluding those with history of diabetes or using insulin or oral hypoglycaemic drugs). We calculated sensitivity and specificity in each survey, and then pooled results using a random-effects model. We assessed the sources of heterogeneity of sensitivity by meta-regressions for study characteristics selected a priori.
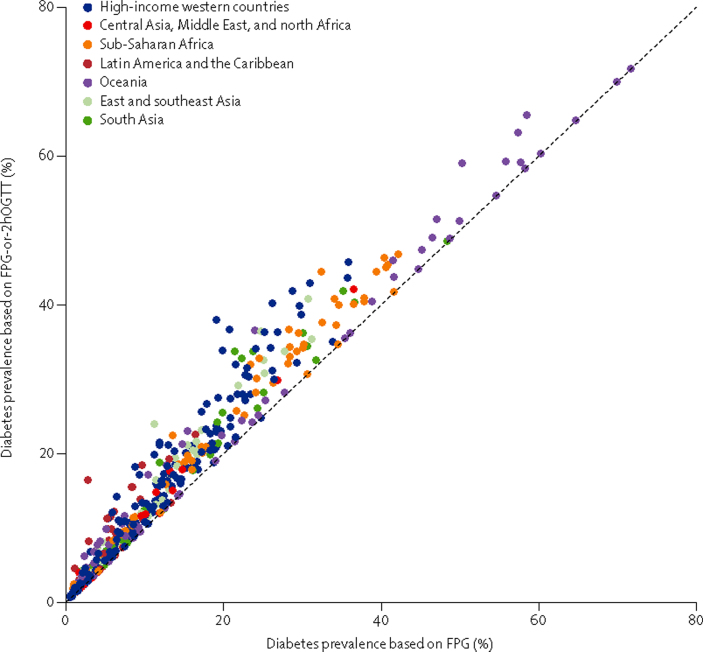
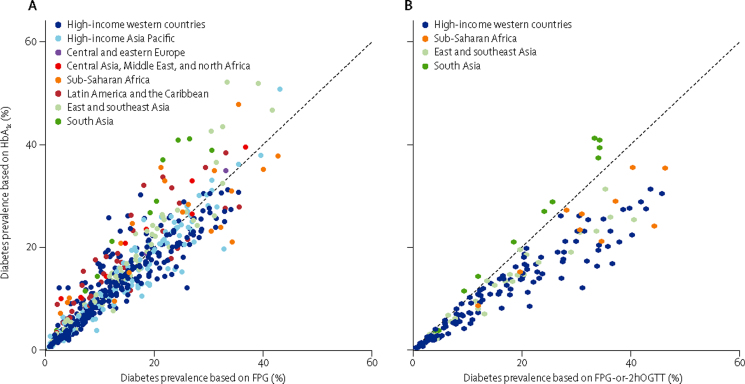
Findings: Population prevalence of diabetes based on FPG-or-2hOGTT was correlated with prevalence based on FPG alone (r=0·98), but was higher by 2-6 percentage points at different prevalence levels. Prevalence based on HbA1c was lower than prevalence based on FPG in 42·8% of age-sex-survey groups and higher in another 41·6%; in the other 15·6%, the two definitions provided similar prevalence estimates. The variation across studies in the relation between glucose-based and HbA1c-based prevalences was partly related to participants' age, followed by natural logarithm of per person gross domestic product, the year of survey, mean BMI, and whether the survey population was national, subnational, or from specific communities. Diabetes defined as HbA1c 6·5% or more had a pooled sensitivity of 52·8% (95% CI 51·3-54·3%) and a pooled specificity of 99·74% (99·71-99·78%) compared with FPG 7·0 mmol/L or more for diagnosing previously undiagnosed participants; sensitivity compared with diabetes defined based on FPG-or-2hOGTT was 30·5% (28·7-32·3%). None of the preselected study-level characteristics explained the heterogeneity in the sensitivity of HbA1c versus FPG.
Interpretation: Different biomarkers and definitions for diabetes can provide different estimates of population prevalence of diabetes, and differentially identify people without previous diagnosis as having diabetes. Using an HbA1c-based definition alone in health surveys will not identify a substantial proportion of previously undiagnosed people who would be considered as having diabetes using a glucose-based test.
Funding: Wellcome Trust, US National Institutes of Health.
Copyright © 2015 NCD Risk Factor Collaboration. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Which biochemical assay is best for measuring diabetes prevalence?Lancet Diabetes Endocrinol. 2015 Aug;3(8):582-3. doi: 10.1016/S2213-8587(15)00203-X. Epub 2015 Jun 21. Lancet Diabetes Endocrinol. 2015. PMID: 26109025 No abstract available.
References
-
- Danaei G, Finucane MM, Lu Y. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2·7 million participants. Lancet. 2011;378:31–40. - PubMed
-
- Kontis V, Mathers CD, Rehm J. Contribution of six risk factors to achieving the 25×25 non-communicable disease mortality reduction target: a modelling study. Lancet. 2014;384:427–437. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- MC_UP_A620_1015/MRC_/Medical Research Council/United Kingdom
- MC_U147585827/MRC_/Medical Research Council/United Kingdom
- MC_UU_12011/2/MRC_/Medical Research Council/United Kingdom
- MC_UP_A620_1014/MRC_/Medical Research Council/United Kingdom
- 100693/WT_/Wellcome Trust/United Kingdom
- 098504/WT_/Wellcome Trust/United Kingdom
- RG/13/16/30528/BHF_/British Heart Foundation/United Kingdom
- MR/M007405/1/MRC_/Medical Research Council/United Kingdom
- MC_U147574245/MRC_/Medical Research Council/United Kingdom
- DK090435/DK/NIDDK NIH HHS/United States
- MC_UU_12019/1/MRC_/Medical Research Council/United Kingdom
- MC_U147585819/MRC_/Medical Research Council/United Kingdom
- RG/08/013/25942/BHF_/British Heart Foundation/United Kingdom
- MC_UU_12011/3/MRC_/Medical Research Council/United Kingdom
- PG/05/046/18730/BHF_/British Heart Foundation/United Kingdom
- MC_U147574218/MRC_/Medical Research Council/United Kingdom
- R01 DK090435/DK/NIDDK NIH HHS/United States
- MR/K006584/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_12011/1/MRC_/Medical Research Council/United Kingdom
- G0400491/MRC_/Medical Research Council/United Kingdom
- MC_UP_A620_1016/MRC_/Medical Research Council/United Kingdom
- MC_U147585824/MRC_/Medical Research Council/United Kingdom
- MR/J000094/1/MRC_/Medical Research Council/United Kingdom
