

Cell-Free DNA Next-Generation Sequencing in Pancreatobiliary Carcinomas
- PMID: 26109333
- PMCID: PMC4592417
- DOI: 10.1158/2159-8290.CD-15-0274
Cell-Free DNA Next-Generation Sequencing in Pancreatobiliary Carcinomas
Abstract
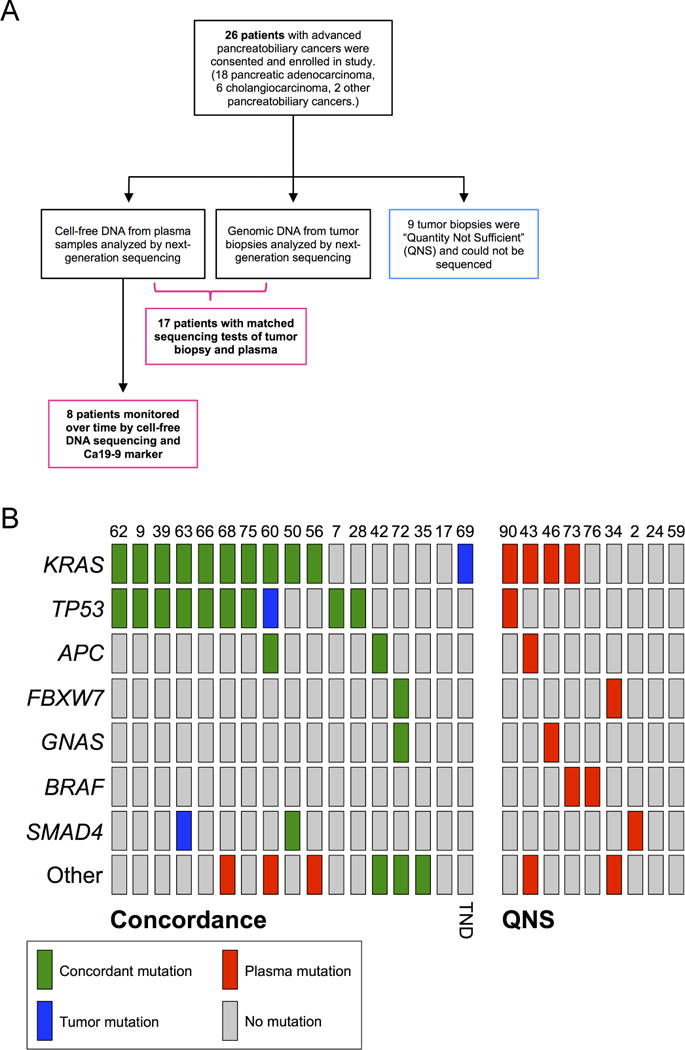
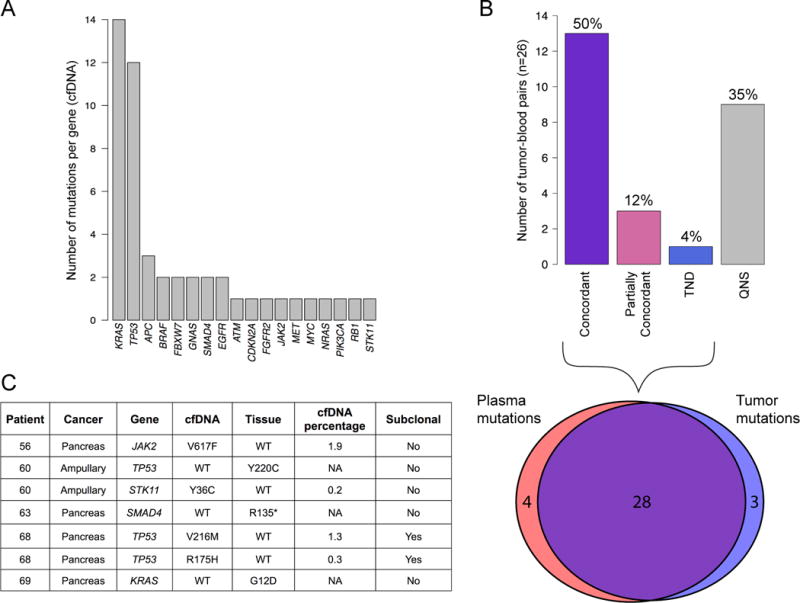
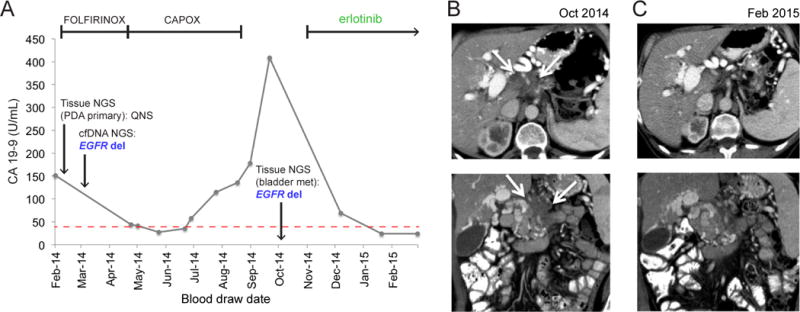
Patients with pancreatic and biliary carcinomas lack personalized treatment options, in part because biopsies are often inadequate for molecular characterization. Cell-free DNA (cfDNA) sequencing may enable a precision oncology approach in this setting. We attempted to prospectively analyze 54 genes in tumor and cfDNA for 26 patients. Tumor sequencing failed in 9 patients (35%). In the remaining 17, 90.3% (95% confidence interval, 73.1%-97.5%) of mutations detected in tumor biopsies were also detected in cfDNA. The diagnostic accuracy of cfDNA sequencing was 97.7%, with 92.3% average sensitivity and 100% specificity across five informative genes. Changes in cfDNA correlated well with tumor marker dynamics in serial sampling (r = 0.93). We demonstrate that cfDNA sequencing is feasible, accurate, and sensitive in identifying tumor-derived mutations without prior knowledge of tumor genotype or the abundance of circulating tumor DNA. cfDNA sequencing should be considered in pancreatobiliary cancer trials where tissue sampling is unsafe, infeasible, or otherwise unsuccessful.
Significance: Precision medicine efforts in biliary and pancreatic cancers have been frustrated by difficulties in obtaining adequate tumor tissue for next-generation sequencing. cfDNA sequencing reliably and accurately detects tumor-derived mutations, paving the way for precision oncology approaches in these deadly diseases.
©2015 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Ryan DP, Hong TS, Bardeesy N. Pancreatic adenocarcinoma. N Engl J Med. 2014;371:2140–1. - PubMed
-
- Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, Brannigan BW, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350:2129–39. - PubMed
-
- Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V, Bajamonde A, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344:783–92. - PubMed
-
- Neesse A, Michl P, Frese KK, Feig C, Cook N, Jacobetz MA, et al. Stromal biology and therapy in pancreatic cancer. Gut. 2011;60:861–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
