

Visual vs Fully Automatic Histogram-Based Assessment of Idiopathic Pulmonary Fibrosis (IPF) Progression Using Sequential Multidetector Computed Tomography (MDCT)
- PMID: 26110421
- PMCID: PMC4482435
- DOI: 10.1371/journal.pone.0130653
Visual vs Fully Automatic Histogram-Based Assessment of Idiopathic Pulmonary Fibrosis (IPF) Progression Using Sequential Multidetector Computed Tomography (MDCT)
Abstract
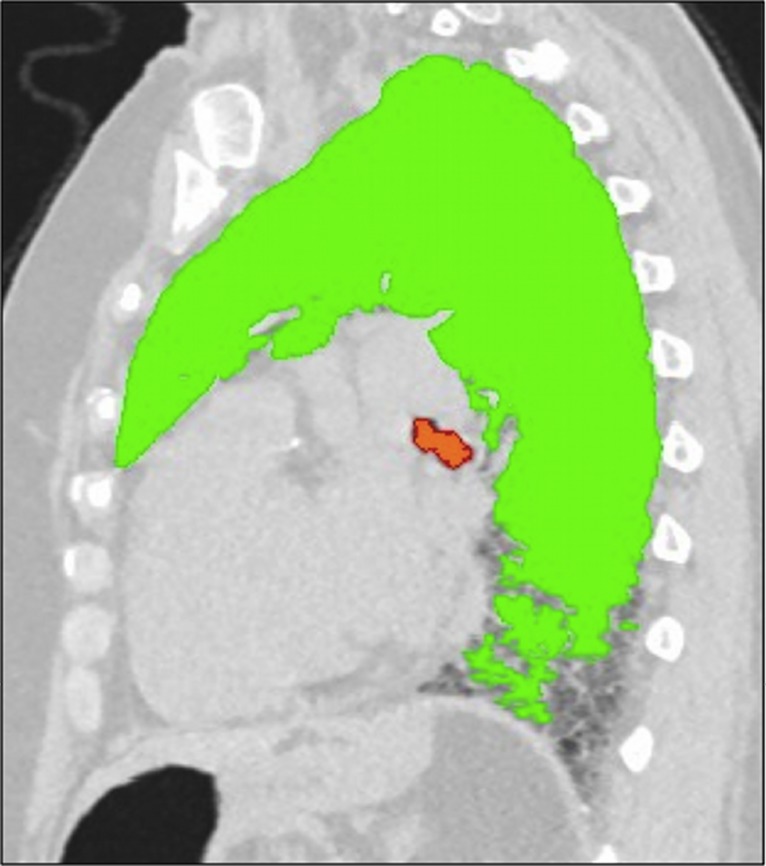
Objectives: To describe changes over time in extent of idiopathic pulmonary fibrosis (IPF) at multidetector computed tomography (MDCT) assessed by semi-quantitative visual scores (VSs) and fully automatic histogram-based quantitative evaluation and to test the relationship between these two methods of quantification.
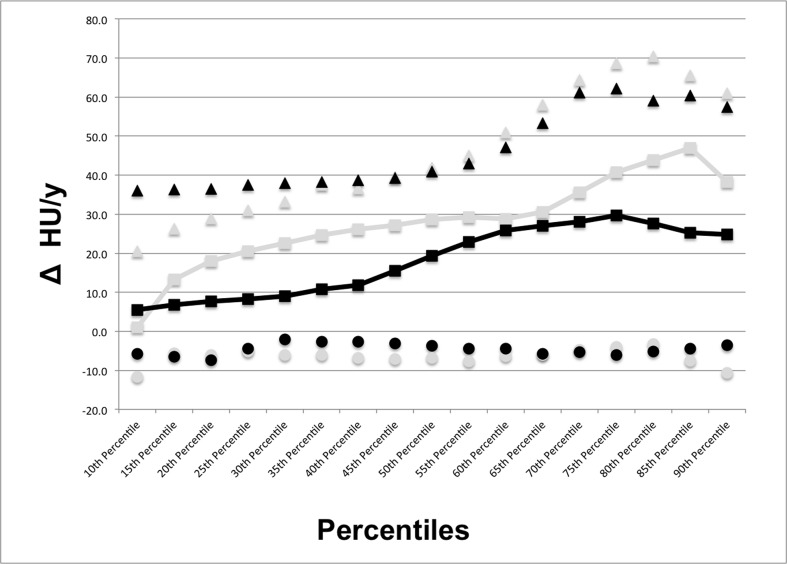
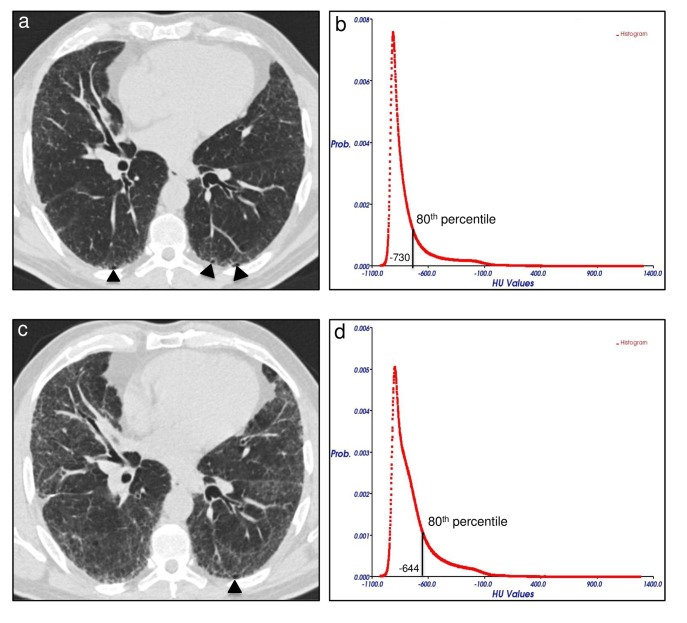
Methods: Forty IPF patients (median age: 70 y, interquartile: 62-75 years; M:F, 33:7) that underwent 2 MDCT at different time points with a median interval of 13 months (interquartile: 10-17 months) were retrospectively evaluated. In-house software YACTA quantified automatically lung density histogram (10th-90th percentile in 5th percentile steps). Longitudinal changes in VSs and in the percentiles of attenuation histogram were obtained in 20 untreated patients and 20 patients treated with pirfenidone. Pearson correlation analysis was used to test the relationship between VSs and selected percentiles.
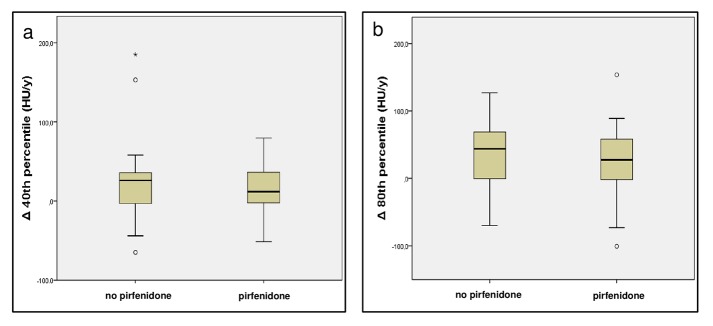
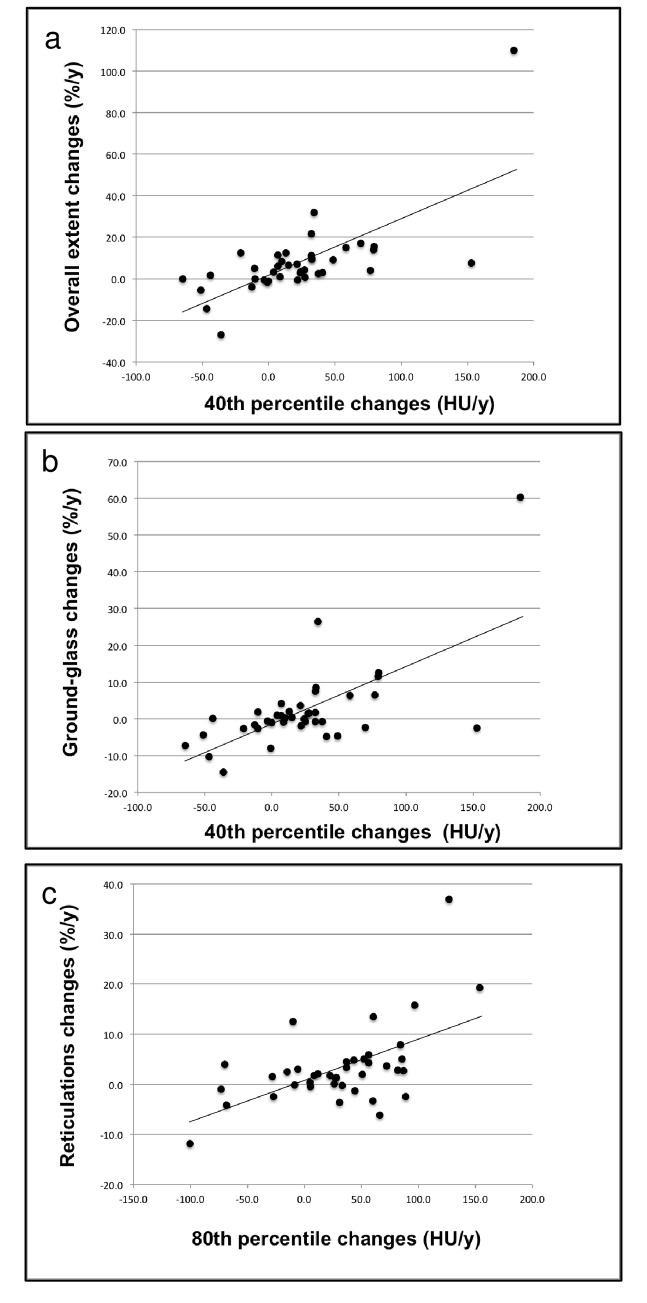
Results: In follow-up MDCT, visual overall extent of parenchymal abnormalities (OE) increased in median by 5%/year (interquartile: 0%/y; +11%/y). Substantial difference was found between treated and untreated patients in HU changes of the 40th and of the 80th percentiles of density histogram. Correlation analysis between VSs and selected percentiles showed higher correlation between the changes (Δ) in OE and Δ 40th percentile (r=0.69; p<0.001) as compared to Δ 80th percentile (r=0.58; p<0.001); closer correlation was found between Δ ground-glass extent and Δ 40th percentile (r=0.66, p<0.001) as compared to Δ 80th percentile (r=0.47, p=0.002), while the Δ reticulations correlated better with the Δ 80th percentile (r=0.56, p<0.001) in comparison to Δ 40th percentile (r=0.43, p=0.003).
Conclusions: There is a relevant and fully automatically measurable difference at MDCT in VSs and in histogram analysis at one year follow-up of IPF patients, whether treated or untreated: Δ 40th percentile might reflect the change in overall extent of lung abnormalities, notably of ground-glass pattern; furthermore Δ 80th percentile might reveal the course of reticular opacities.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
