

Prominent vessel sign on susceptibility-weighted imaging in acute stroke: prediction of infarct growth and clinical outcome
- PMID: 26110628
- PMCID: PMC4481350
- DOI: 10.1371/journal.pone.0131118
Prominent vessel sign on susceptibility-weighted imaging in acute stroke: prediction of infarct growth and clinical outcome
Abstract
Background and purpose: Predicting the risk of further infarct growth in stroke patients is critical to therapeutic decision making. We aimed to predict early infarct growth and clinical outcome from prominent vessel sign (PVS) identified on the first susceptibility-weighted image (SWI) after acute stroke.
Materials and methods: Twenty-two patients with middle cerebral artery (MCA) infarction had diffusion-weighted imaging, SWI, MR angiography, and clinical evaluation using the National Institutes of Health Stroke Scale at 7-60 hours and 5-14 days after stroke onset. Late-stage clinical evaluation at 1 and 3 months used the modified Rankin Scale. The infarct area and growth were scored from 10 (none) to 0 (infarct or growth in all 10 zones) using the Alberta Stroke Program Early CT Score (ASPECTS) system.
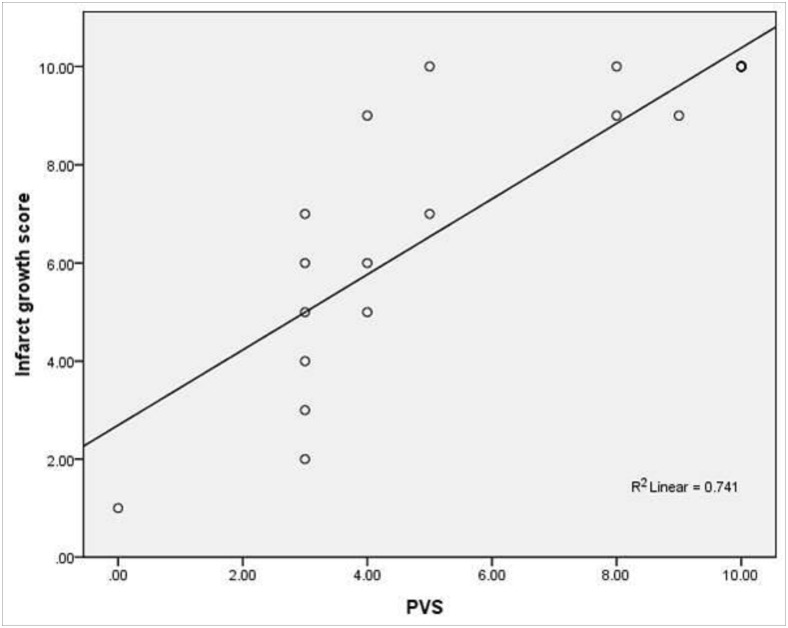
Results: Infarct growth on the second MRI occurred in 13 of 15 patients with PVS on the first MRI and not in any patient without PVS (n=7; r=0.86, P<0.001). The extent of PVS was significantly correlated with infarct growth (r=0.82, P<0.001) and early-stage outcome (P=0.02). No between-group difference in late-stage clinical outcome was found.
Conclusion: PVS on the first SWI after acute MCA territory stroke is a useful predictor of early infarct growth. Extensive PVS within the large MCA territory is related to poor early-stage outcome and could be useful for clinical assessment of stroke.
Conflict of interest statement
Figures



References
-
- Sobesky J, Zaro Weber O, Lehnhardt FG, Hesselmann V, Neveling M, Jacobs A, et al. Does the mismatch match the penumbra? MRI and PET in early ischemic stroke. Stroke 2005;36:980–5 - PubMed
-
- Heiss WD. Ischemic penumbra: evidence from functional imaging in man. J Cereb Blood Flow Metab 2000;20:1276–93 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
