

Viral Infection of Tumors Overcomes Resistance to PD-1-immunotherapy by Broadening Neoantigenome-directed T-cell Responses
- PMID: 26112079
- PMCID: PMC4817928
- DOI: 10.1038/mt.2015.115
Viral Infection of Tumors Overcomes Resistance to PD-1-immunotherapy by Broadening Neoantigenome-directed T-cell Responses
Abstract
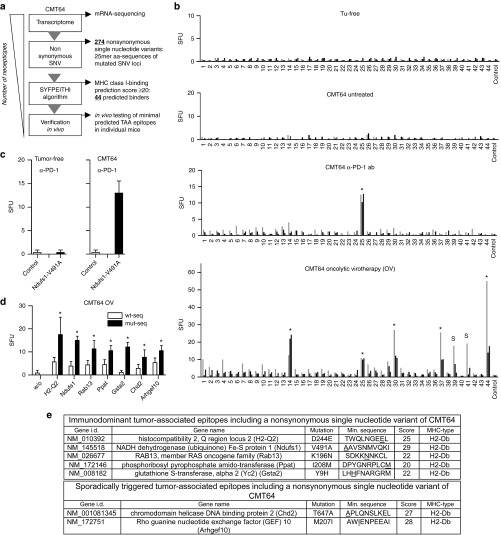
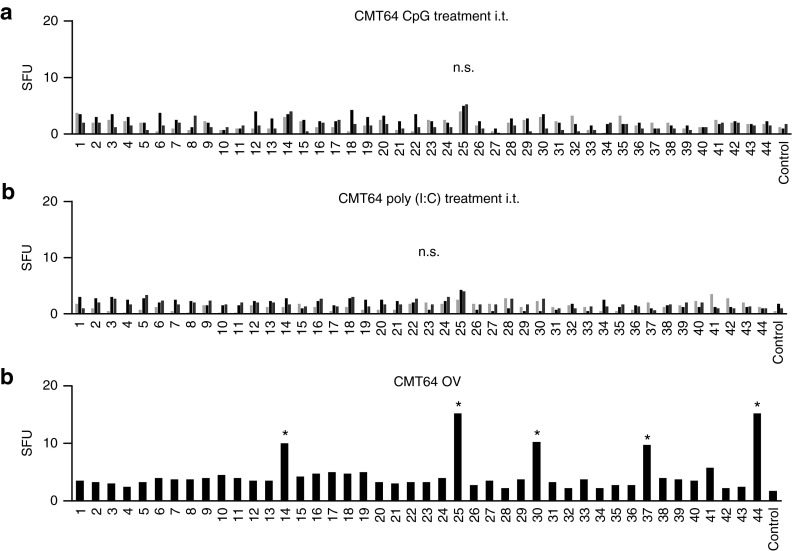
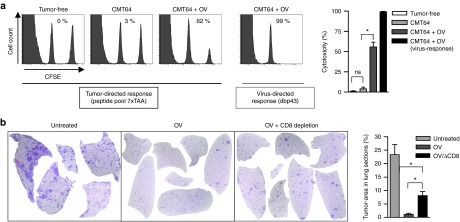
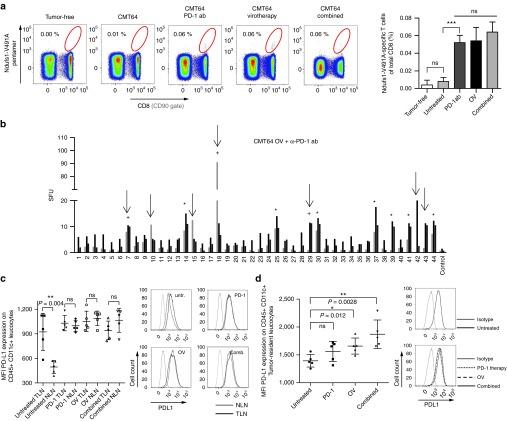
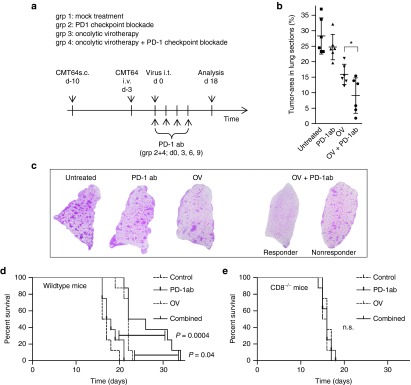
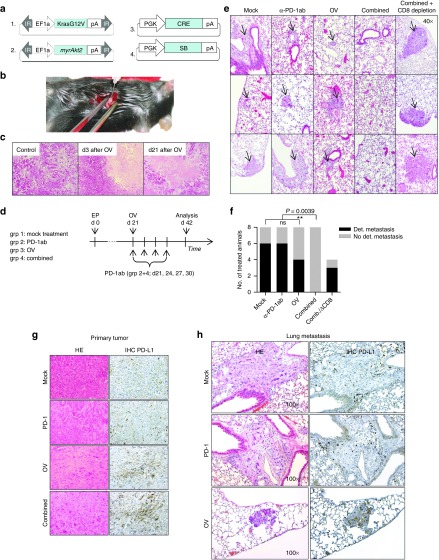
There is evidence that viral oncolysis is synergistic with immune checkpoint inhibition in cancer therapy but the underlying mechanisms are unclear. Here, we investigated whether local viral infection of malignant tumors is capable of overcoming systemic resistance to PD-1-immunotherapy by modulating the spectrum of tumor-directed CD8 T-cells. To focus on neoantigen-specific CD8 T-cell responses, we performed transcriptomic sequencing of PD-1-resistant CMT64 lung adenocarcinoma cells followed by algorithm-based neoepitope prediction. Investigations on neoepitope-specific T-cell responses in tumor-bearing mice demonstrated that PD-1 immunotherapy was insufficient whereas viral oncolysis elicited cytotoxic T-cell responses to a conserved panel of neoepitopes. After combined treatment, we observed that PD-1-blockade did not affect the magnitude of oncolysis-mediated antitumoral immune responses but a broader spectrum of T-cell responses including additional neoepitopes was observed. Oncolysis of the primary tumor significantly abrogated systemic resistance to PD-1-immunotherapy leading to improved elimination of disseminated lung tumors. Our observations were confirmed in a transgenic murine model of liver cancer where viral oncolysis strongly induced PD-L1 expression in primary liver tumors and lung metastasis. Furthermore, we demonstrated that combined treatment completely inhibited dissemination in a CD8 T-cell-dependent manner. Therefore, our results strongly recommend further evaluation of virotherapy and concomitant PD-1 immunotherapy in clinical studies.
Figures
References
-
- Lynch, TJ, Bondarenko, I, Luft, A, Serwatowski, P, Barlesi, F, Chacko, R et al. (2012). Ipilimumab in combination with paclitaxel and carboplatin as first-line treatment in stage IIIB/IV non-small-cell lung cancer: results from a randomized, double-blind, multicenter phase II study. J Clin Oncol 30: 2046–2054. - PubMed
-
- Powles, T, Eder, JP, Fine, GD, Braiteh, FS, Loriot, Y, Cruz, C et al. (2014). MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature 515: 558–562. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
