

Preliminary experience using milnacipran in patients with juvenile fibromyalgia: lessons from a clinical trial program
- PMID: 26112278
- PMCID: PMC4480575
- DOI: 10.1186/s12969-015-0025-9
Preliminary experience using milnacipran in patients with juvenile fibromyalgia: lessons from a clinical trial program
Abstract
Background: There are no approved medications for juvenile fibromyalgia (JFM), a disorder that is often under-diagnosed. The effects of milnacipran, a drug approved for the management of fibromyalgia (FM) in adults, was assessed in a clinical trial program for JFM.
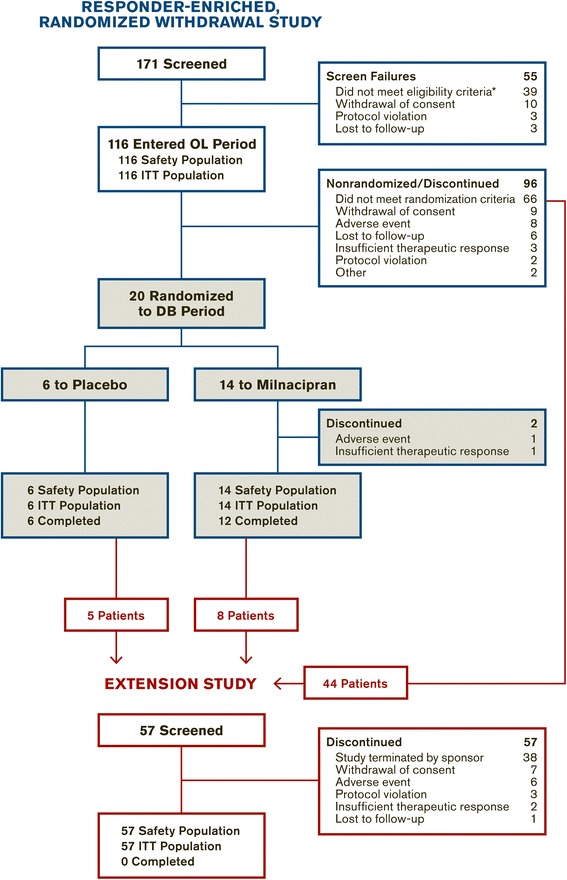
Methods: Patients, ages 13-17 years who met the Yunus and Masi criteria for JFM and/or 1990 American College of Rheumatology criteria for FM, were enrolled in a responder-enriched, randomized withdrawal trial. After receiving open-label milnacipran (8 weeks), patients with ≥50 % improvement in pain underwent double-blind randomization (1:2) to either placebo or continuing treatment with milnacipran (8 weeks). All patients, including those who did not meet the randomization criteria for double-blind withdrawal, were allowed to enter an extension study with open-label milnacipran (up to 52 weeks). The primary endpoint was loss of therapeutic response (LTR) during the double-blind period. Additional outcome measures included the Patient Global Impression of Severity (PGIS), Pediatric Quality of Life Inventory (PedsQL: Generic Core Scales, Multidimensional Fatigue Scale), and Multidimensional Anxiety Scale for Children (MASC). Safety assessments included adverse events (AEs), vital signs, electrocardiograms, and laboratory tests.
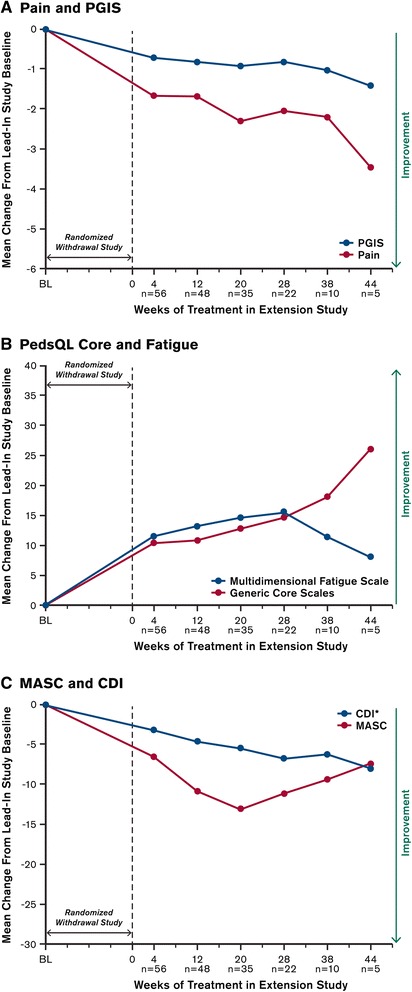
Results: The milnacipran program was terminated early due to low enrollment. Because only 20 patients were randomized into the double-blind withdrawal period, statistical analyses were not conducted for the LTR endpoint. However, 116 patients entered the open-label period of the initial study and 57 participated in the open-label extension study. Their experience provides preliminary information about the use of milnacipran in JFM patients. During both open-label periods, there were mean improvements in pain severity, PGIC, PedsQL, and MASC scores. No unexpected safety issues were detected. The most commonly reported treatment-emergent AEs were nausea, headache, vomiting, and dizziness. Mean increases in heart rate and blood pressure were observed, and were consistent with the AE profile in adults with FM.
Conclusions: The open-label findings provide preliminary evidence that milnacipran may improve symptoms of JFM, with a safety and tolerability profile that is consistent with the experience in adult FM patients. Future trial designs for JFM should consider the relatively low recognition of this condition compared to adult FM and the difficulties with enrollment.
Trial registration: NCT01328002 ; NCT01331109.
Figures
References
-
- Clark P, Burgos-Vargas R, Medina-Palma C, Lavielle P, Marina FF. Prevalence of fibromyalgia in children: a clinical study of Mexican children. J Rheumatol. 1998;25:2009–14. - PubMed
-
- Durmaz Y, Alayli G, Canbaz S, Zahiroglu Y, Bilgici A, Ilhanli I, et al. Prevalence of juvenile fibromyalgia syndrome in an urban population of Turkish adolescents: impact on depressive symptoms, quality of life and school performance. Chin Med J (Engl) 2013;126:3705–11. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
