

Implementation of an electronic fingerprint-linked data collection system: a feasibility and acceptability study among Zambian female sex workers
- PMID: 26115656
- PMCID: PMC4489038
- DOI: 10.1186/s12992-015-0114-z
Implementation of an electronic fingerprint-linked data collection system: a feasibility and acceptability study among Zambian female sex workers
Abstract
Background: Patient identification within and between health services is an operational challenge in many resource-limited settings. When following HIV risk groups for service provision and in the context of vaccine trials, patient misidentification can harm patient care and bias trial outcomes. Electronic fingerprinting has been proposed to identify patients over time and link patient data between health services. The objective of this study was to determine 1) the feasibility of implementing an electronic-fingerprint linked data capture system in Zambia and 2) the acceptability of this system among a key HIV risk group: female sex workers (FSWs).
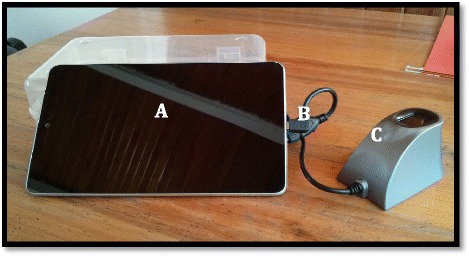
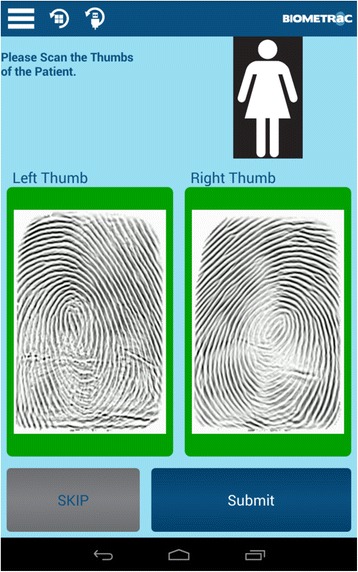
Methods: Working with Biometrac, a US-based company providing biometric-linked healthcare platforms, an electronic fingerprint-linked data capture system was developed for use by field recruiters among Zambian FSWs. We evaluated the technical feasibility of the system for use in the field in Zambia and conducted a pilot study to determine the acceptability of the system, as well as barriers to uptake, among FSWs.
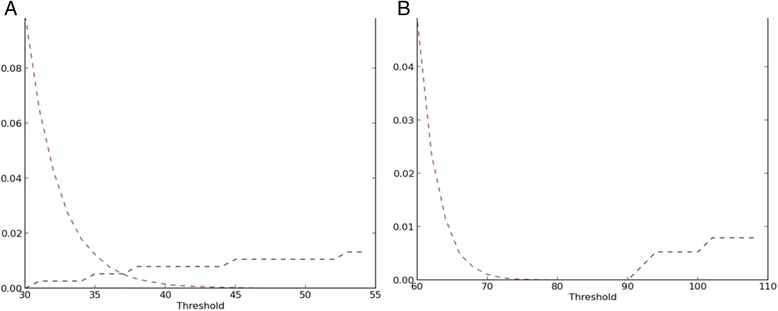
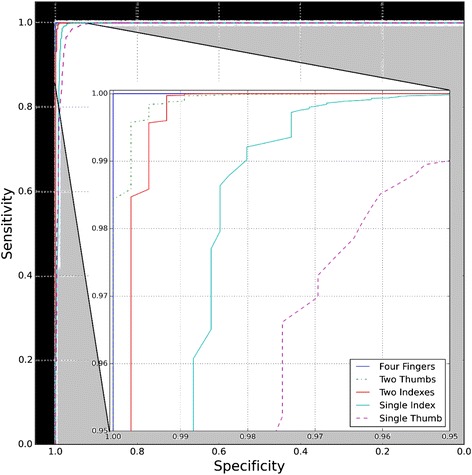
Results: We found that implementation of an electronic fingerprint-linked patient tracking and data collection system was feasible in this relatively resource-limited setting (false fingerprint matching rate of 1/1000 and false rejection rate of <1/10,000) and was acceptable among FSWs in a clinic setting (2% refusals). However, our data indicate that less than half of FSWs are comfortable providing an electronic fingerprint when recruited while they are working. The most common reasons cited for not providing a fingerprint (lack of privacy/confidentiality issues while at work, typically at bars or lodges) could be addressed by recruiting women during less busy hours, in their own homes, in the presence of "Queen Mothers" (FSW organizers), or in the presence of a FSW that has already been fingerprinted.
Conclusions: Our findings have major implications for key population research and improved health services provision. However, more work needs to be done to increase the acceptability of the electronic fingerprint-linked data capture system during field recruitment. This study indicated several potential avenues that will be explored to increase acceptability.
Figures
References
-
- Patient Identification. [http://www.who.int/patientsafety/solutions/patientsafety/PS-Solution2.pdf]
-
- Guidance on Couples HIV Testing and Counselling Including Antiretroviral Therapy for Treatment and Prevention in Serodiscordant Couples: Recommendations for a Public Health Approach. [http://apps.who.int/iris/bitstream/10665/44646/1/9789241501972_eng.pdf] - PubMed
-
- Vermund SH, Fidler SJ, Ayles H, Beyers N, Hayes RJ. Can combination prevention strategies reduce HIV transmission in generalized epidemic settings in Africa? The HPTN 071 (PopART) study plan in South Africa and Zambia. J Acquir Immune Defic Syndr. 2013;63(Suppl 2):S221–7. doi: 10.1097/QAI.0b013e318299c3f4. - DOI - PMC - PubMed
-
- Aspden P, Wolcott JA, Bootman JL, Cronenwett LR, editors. Preventing Medication Errors. Washington, DC: Institute of Medicine; 2006.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
