

Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): overall survival results of a phase 3 randomised trial
- PMID: 26115797
- PMCID: PMC4648090
- DOI: 10.1016/S1470-2045(15)00086-8
Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): overall survival results of a phase 3 randomised trial
Abstract
Background: The ICON7 trial previously reported improved progression-free survival in women with ovarian cancer with the addition of bevacizumab to standard chemotherapy, with the greatest effect in patients at high risk of disease progression. We report the final overall survival results of the trial.
Methods: ICON7 was an international, phase 3, open-label, randomised trial undertaken at 263 centres in 11 countries across Europe, Canada, Australia and New Zealand. Eligible adult women with newly diagnosed ovarian cancer that was either high-risk early-stage disease (International Federation of Gynecology and Obstetrics [FIGO] stage I-IIa, grade 3 or clear cell histology) or more advanced disease (FIGO stage IIb-IV), with an Eastern Cooperative Oncology Group performance status of 0-2, were enrolled and randomly assigned in a 1:1 ratio to standard chemotherapy (six 3-weekly cycles of intravenous carboplatin [AUC 5 or 6] and paclitaxel 175 mg/m(2) of body surface area) or the same chemotherapy regimen plus bevacizumab 7·5 mg per kg bodyweight intravenously every 3 weeks, given concurrently and continued with up to 12 further 3-weekly cycles of maintenance therapy. Randomisation was done by a minimisation algorithm stratified by FIGO stage, residual disease, interval between surgery and chemotherapy, and Gynecologic Cancer InterGroup group. The primary endpoint was progression-free survival; the study was also powered to detect a difference in overall survival. Analysis was by intention to treat. This trial is registered as an International Standard Randomised Controlled Trial, number ISRCTN91273375.
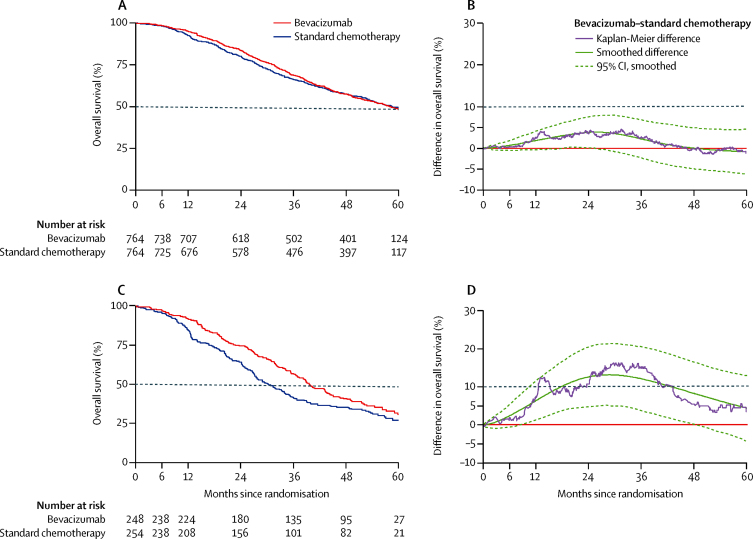
Findings: Between Dec 18, 2006, and Feb 16, 2009, 1528 women were enrolled and randomly assigned to receive chemotherapy (n=764) or chemotherapy plus bevacizumab (n=764). Median follow-up at the end of the trial on March 31, 2013, was 48·9 months (IQR 26·6-56·2), at which point 714 patients had died (352 in the chemotherapy group and 362 in the bevacizumab group). Our results showed evidence of non-proportional hazards, so we used the difference in restricted mean survival time as the primary estimate of effect. No overall survival benefit of bevacizumab was recorded (restricted mean survival time 44·6 months [95% CI 43·2-45·9] in the standard chemotherapy group vs 45·5 months [44·2-46·7] in the bevacizumab group; log-rank p=0·85). In an exploratory analysis of a predefined subgroup of 502 patients with poor prognosis disease, 332 (66%) died (174 in the standard chemotherapy group and 158 in the bevacizumab group), and a significant difference in overall survival was noted between women who received bevacizumab plus chemotherapy and those who received chemotherapy alone (restricted mean survival time 34·5 months [95% CI 32·0-37·0] with standard chemotherapy vs 39·3 months [37·0-41·7] with bevacizumab; log-rank p=0·03). However, in non-high-risk patients, the restricted mean survival time did not differ significantly between the two treatment groups (49·7 months [95% CI 48·3-51·1]) in the standard chemotherapy group vs 48·4 months [47·0-49·9] in the bevacizumab group; p=0·20). An updated analysis of progression-free survival showed no difference between treatment groups. During extended follow-up, one further treatment-related grade 3 event (gastrointestinal fistula in a bevacizumab-treated patient), three grade 2 treatment-related events (cardiac failure, sarcoidosis, and foot fracture, all in bevacizumab-treated patients), and one grade 1 treatment-related event (vaginal haemorrhage, in a patient treated with standard chemotherapy) were reported.
Interpretation: Bevacizumab, added to platinum-based chemotherapy, did not increase overall survival in the study population as a whole. However, an overall survival benefit was recorded in poor-prognosis patients, which is concordant with the progression-free survival results from ICON7 and GOG-218, and provides further evidence towards the optimum use of bevacizumab in the treatment of ovarian cancer.
Funding: The National Institute for Health Research through the UK National Cancer Research Network, the Medical Research Council, and Roche.
Copyright © 2015 Oza et al. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd.. All rights reserved.
Figures


Comment in
-
Bevacizumab in newly diagnosed ovarian cancer.Lancet Oncol. 2015 Aug;16(8):876-8. doi: 10.1016/S1470-2045(15)00064-9. Epub 2015 Jun 23. Lancet Oncol. 2015. PMID: 26115795 No abstract available.
-
Discordance between the results and conclusions of ICON7 - Authors' reply.Lancet Oncol. 2015 Oct;16(13):e478-9. doi: 10.1016/S1470-2045(15)00311-3. Lancet Oncol. 2015. PMID: 26433820 No abstract available.
-
Discordance between the results and conclusions of ICON7.Lancet Oncol. 2015 Oct;16(13):e478. doi: 10.1016/S1470-2045(15)00283-1. Lancet Oncol. 2015. PMID: 26433821 No abstract available.
References
-
- International Agency for Research on Cancer GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012. http://globocan.iarc.fr/Pages/bar_sex_pop_sel.aspx (accessed Aug 8, 2014).
-
- De Angelis R, Sant M, Coleman MP. Cancer survival in Europe 1999-2007 by country and age: results of EUROCARE-5-a population-based study. Lancet Oncol. 2014;15:23–34. - PubMed
-
- Stuart GC, Kitchener H, Bacon M. 2010 Gynecologic Cancer InterGroup (GCIG) consensus statement on clinical trials in ovarian cancer: report from the Fourth Ovarian Cancer Consensus Conference. Int J Gynecol Cancer. 2011;21:750–755. - PubMed
-
- Folkman J. Tumor angiogenesis: therapeutic implications. N Engl J Med. 1971;285:1182–1186. - PubMed
-
- Burger RA, Brady MF, Bookman MA. Incorporation of bevacizumab in the primary treatment of ovarian cancer. N Engl J Med. 2011;365:2473–2483. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
