

Firearm injuries in the United States
- PMID: 26116133
- PMCID: PMC4700838
- DOI: 10.1016/j.ypmed.2015.06.002
Firearm injuries in the United States
Abstract
Objective: This paper examines the epidemiology of fatal and nonfatal firearm violence in the United States. Trends over two decades in homicide, assault, self-directed and unintentional firearm injuries are described along with current demographic characteristics of victimization and health impact.
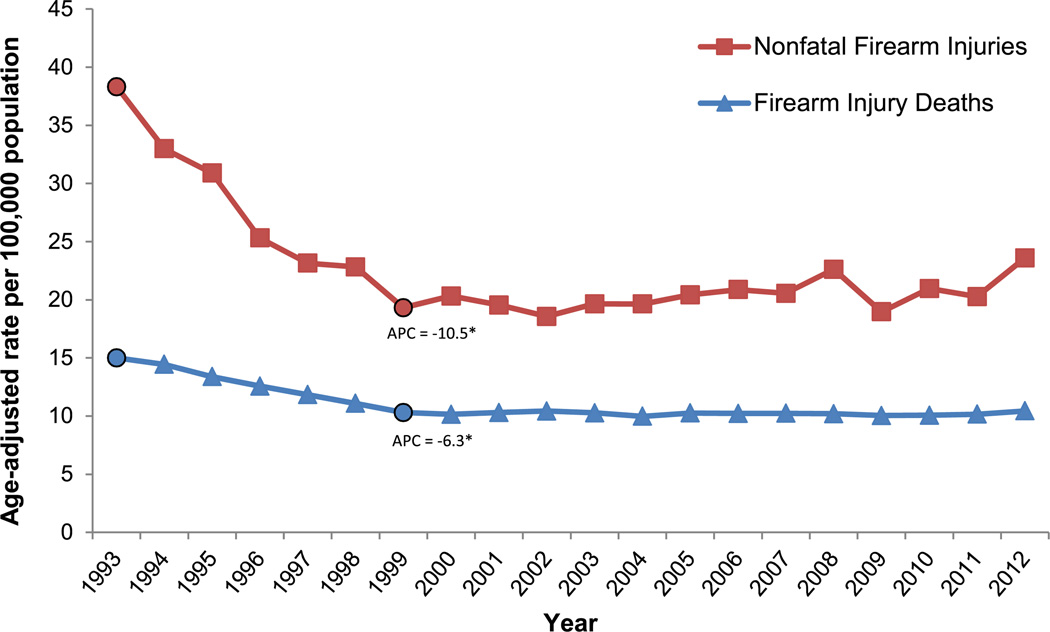
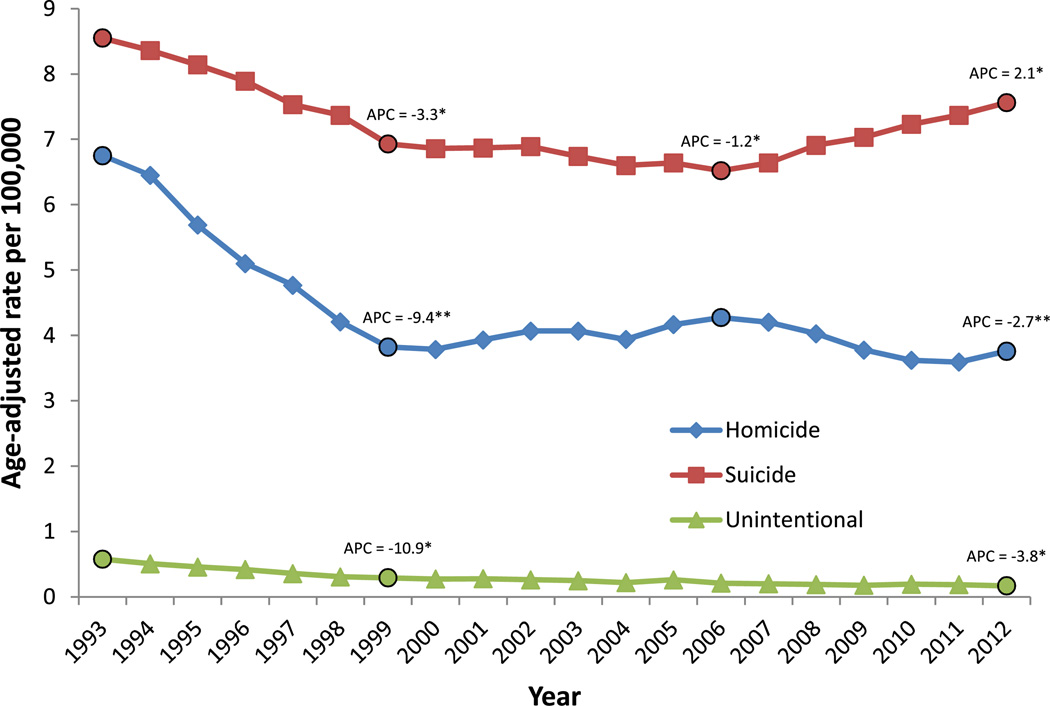
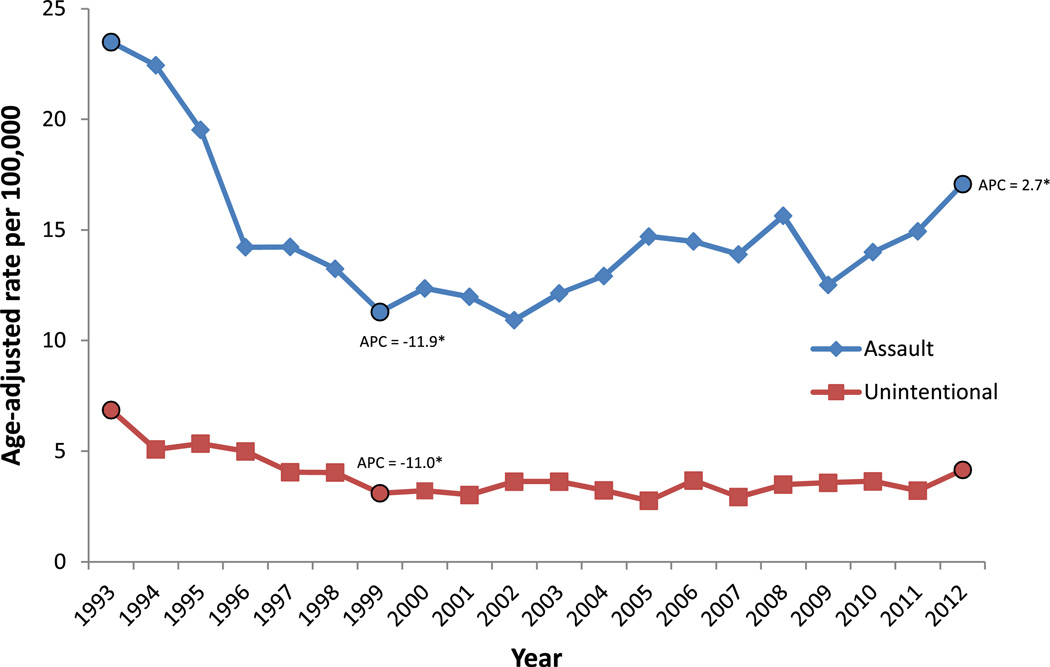
Method: Fatal firearm injury data were obtained from the National Vital Statistics System (NVSS). Nonfatal firearm injury data were obtained from the National Electronic Injury Surveillance System (NEISS). Trends were tested using Joinpoint regression analyses. CDC Cost of Injury modules were used to estimate costs associated with firearm deaths and injuries.
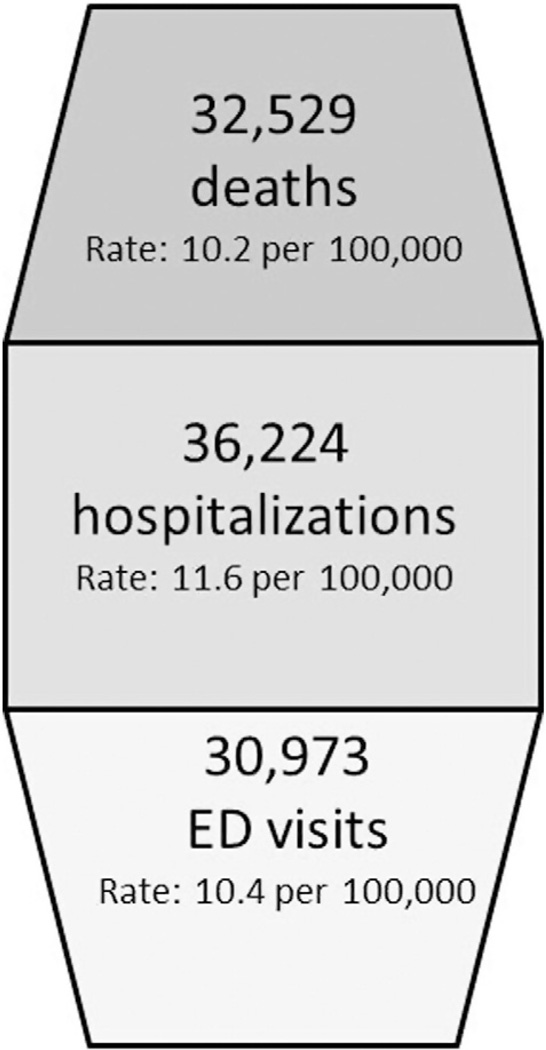
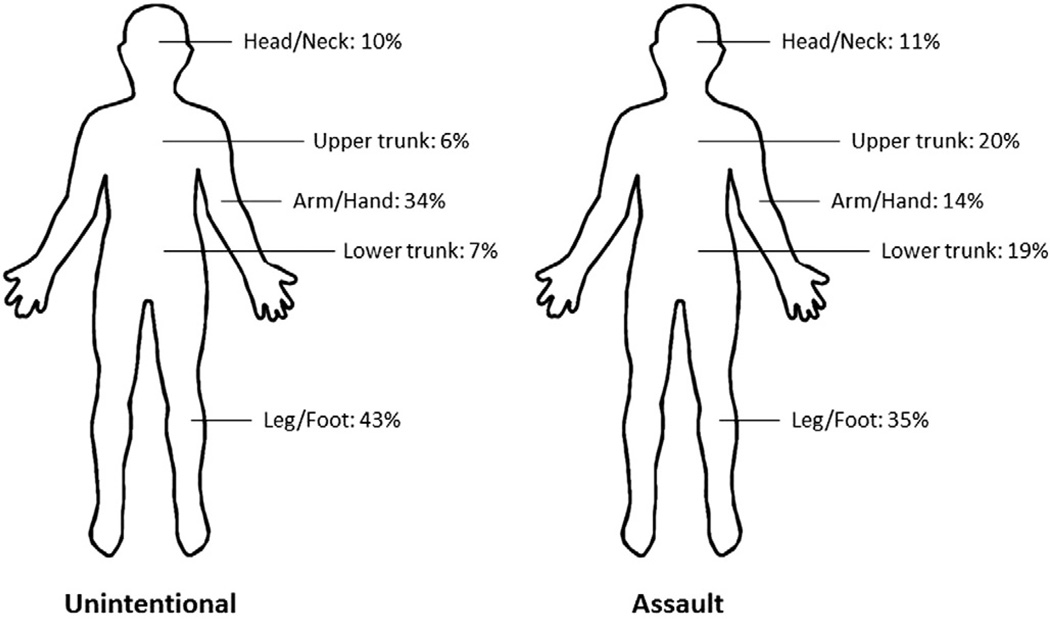
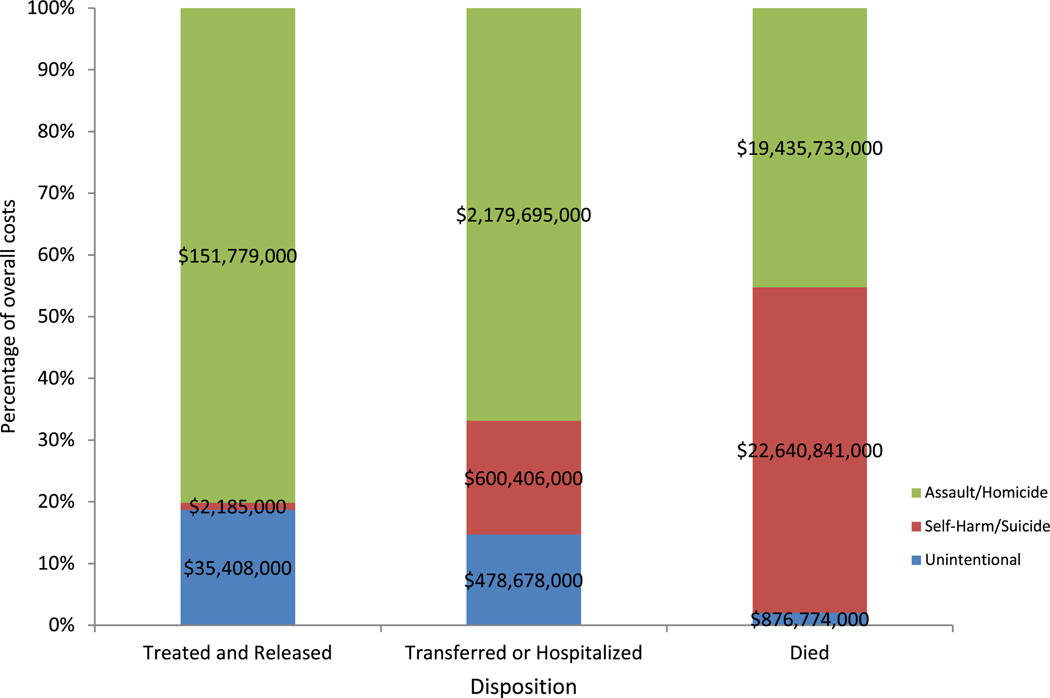
Results: More than 32,000 persons die and over 67,000 persons are injured by firearms each year. Case fatality rates are highest for self-harm related firearm injuries, followed by assault-related injuries. Males, racial/ethnic minority populations, and young Americans (with the exception of firearm suicide) are disproportionately affected. The severity of such injuries is distributed relatively evenly across outcomes from outpatient treatment to hospitalization to death. Firearm injuries result in over $48 billion in medical and work loss costs annually, particularly fatal firearm injuries. From 1993 to 1999, rates of firearm violence declined significantly. Declines were seen in both fatal and nonfatal firearm violence and across all types of intent. While unintentional firearm deaths continued to decline from 2000 to 2012, firearm suicides increased and nonfatal firearm assaults increased to their highest level since 1995.
Conclusion: Firearm injuries are an important public health problem in the United States, contributing substantially each year to premature death, illness, and disability. Understanding the nature and impact of the problem is only a first step toward preventing firearm violence. A science-driven approach to understand risk and protective factors and identify effective solutions is key to achieving measurable reductions in firearm violence.
Keywords: Epidemiology; Firearms; Violence.
Published by Elsevier Inc.
Conflict of interest statement
The authors declare that there are no conflicts of interests.
Figures
References
-
- American Psychological Association. Gun violence: prediction, prevention, and policy. 2013 Retrieved from. http://www.apa.org/pubs/info/reports/gun-violence-prevention.aspx.
-
- Anderson RN, Minino AM, Hoyert DL, Rosenberg HM. National Vital Statistics Reports. 2. Vol. 49. Hyattsville, Maryland: National Center for Health Statistics; 2001. Comparability of cause of death between ICD-9 and ICD-10: preliminary estimates. - PubMed
-
- Arias E, Schauman WS, Eschbach K, Sorlie PD, Backlund E. The validity of race and Hispanic origin reporting on death certificates in the United States. Vital Health Stat. 2008;2(148) - PubMed
-
- Blissitt P. Care of the critically ill patient with penetrating head injury. Crit. Care Nurs. Clin. North Am. 2006;18(3):321–332. - PubMed
-
- Blumstein R. Youth, guns, and violent crime. Future Child. 2002;19(2):39–53. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
