

Improved Natural Killer cell activity and retained anti-tumor CD8(+) T cell responses contribute to the induction of a pathological complete response in HER2-positive breast cancer patients undergoing neoadjuvant chemotherapy
- PMID: 26116238
- PMCID: PMC4483222
- DOI: 10.1186/s12967-015-0567-0
Improved Natural Killer cell activity and retained anti-tumor CD8(+) T cell responses contribute to the induction of a pathological complete response in HER2-positive breast cancer patients undergoing neoadjuvant chemotherapy
Abstract
Background: Locally advanced HER2-overexpressing breast cancer (BC) patients achieve a high rate of pathological complete responses (pCR) after neoadjuvant chemotherapy (NC). The apparently unaltered immune proficiency of these patients together with the immune-modulating activities of NC drugs suggest a potential contribution of host immunity in mediating clinical responses. We thus performed an extensive immunomonitoring in locally advanced BC patients undergoing NC to identify immunological correlates of pCR induction.
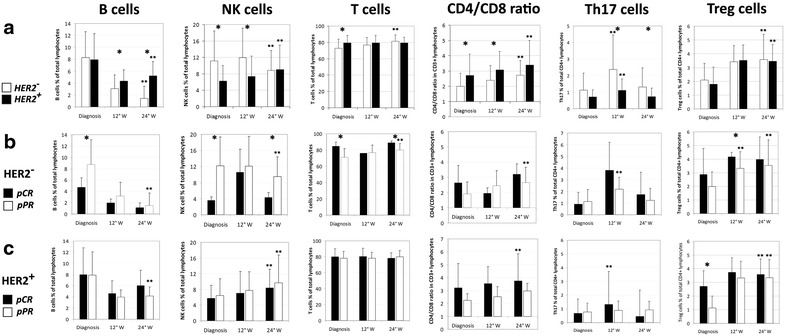
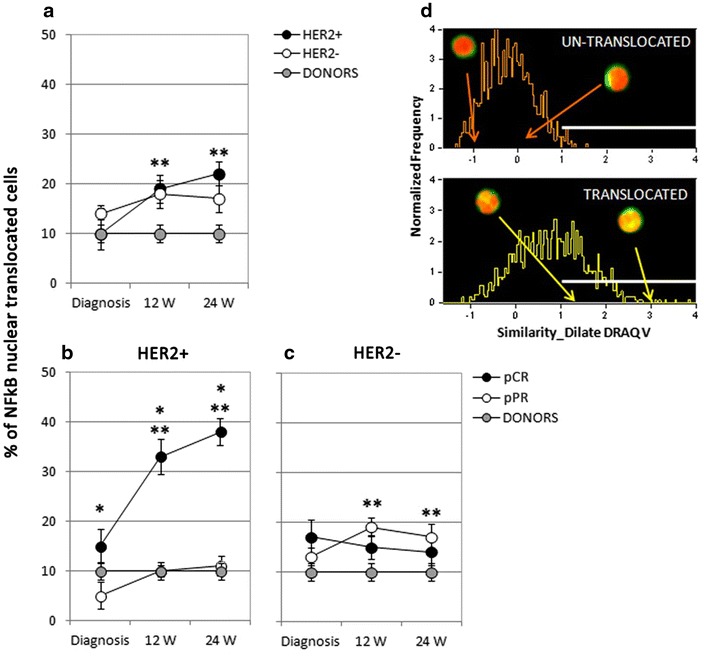
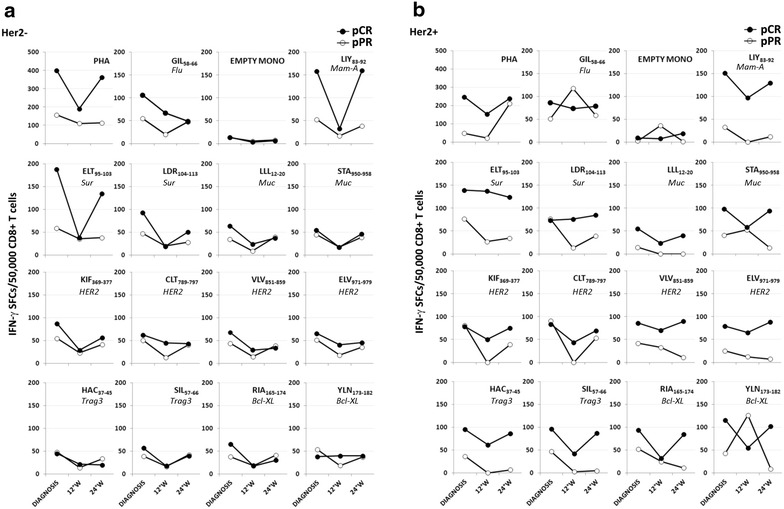
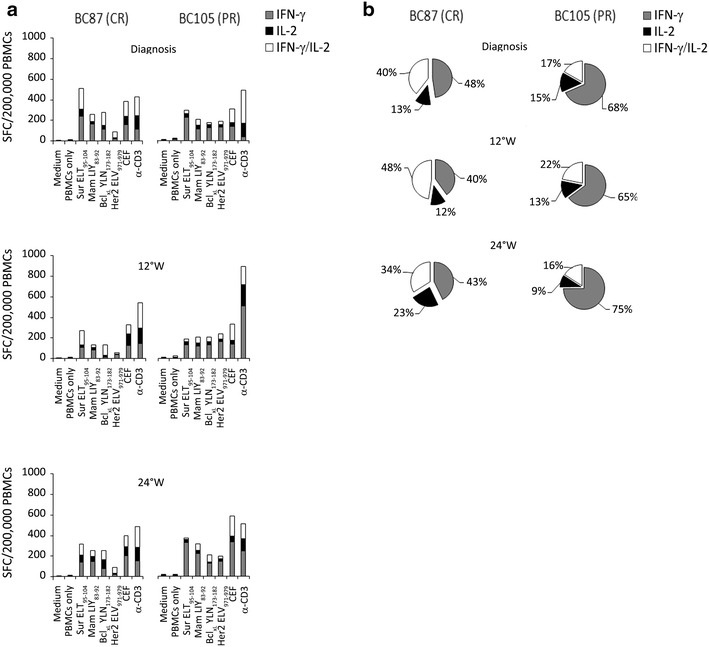
Methods: The immune profile of 40 HER2-positive and 38 HER2-negative BC patients was characterized at diagnosis and throughout NC (Paclitaxel and Trastuzumab, or Docetaxel and Epirubicin, respectively). The percentages of circulating immune cell subsets including T and B lymphocytes, Natural Killer (NK) cells, regulatory T cells, T helper 17 lymphocytes, were quantified by multiparametric flow cytometry. NK cells functional activity was evaluated through the analysis of NF-kB nuclear translocation by Multispectral flow cytometry, and with the in vitro monitoring of Trastuzumab-mediated antibody-dependent cell cytotoxicity (ADCC). CD8(+) T cell responses against six different tumor-associated antigens (TAA) were characterized by IFN-γ ELISPOT and IFN-γ/IL-2 DualSpot assays.
Results: After NC, HER2-positive patients showed a significant increase in the number of NK cells and regulatory T cells irrespective of the pathological response, whereas patients undergoing a pCR disclosed higher percentages of T helper 17 cells. Notably, a significant increase in the number of activated NK cells was observed only in HER2-positive patients achieving a pCR. Characterization of anti-tumor T cell responses highlighted sustained levels of CD8(+) T cells specific for survivin and mammaglobin-A throughout NC in patients undergoing a pCR in both arms. Moreover, HER2-positive patients achieving a pCR were characterized by a multi-epitopic and polyfunctional anti-tumor T cell response, markedly reduced in case of partial response.
Conclusions: These results indicate that maintenance of functional T cell responses against selected antigens and improvement of NK cell proficiency during NC are probably critical requirements for pCR induction, especially in HER2-positive BC patients. Trail registration:
Trial registration number: NCT02307227, registered on ClinicalTrials.gov ( http://www.clinicaltrials.gov , November 26, 2014).
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
