

The effects of telemedicine on racial and ethnic disparities in access to acute stroke care
- PMID: 26116854
- PMCID: PMC4948296
- DOI: 10.1177/1357633X15589534
The effects of telemedicine on racial and ethnic disparities in access to acute stroke care
Abstract
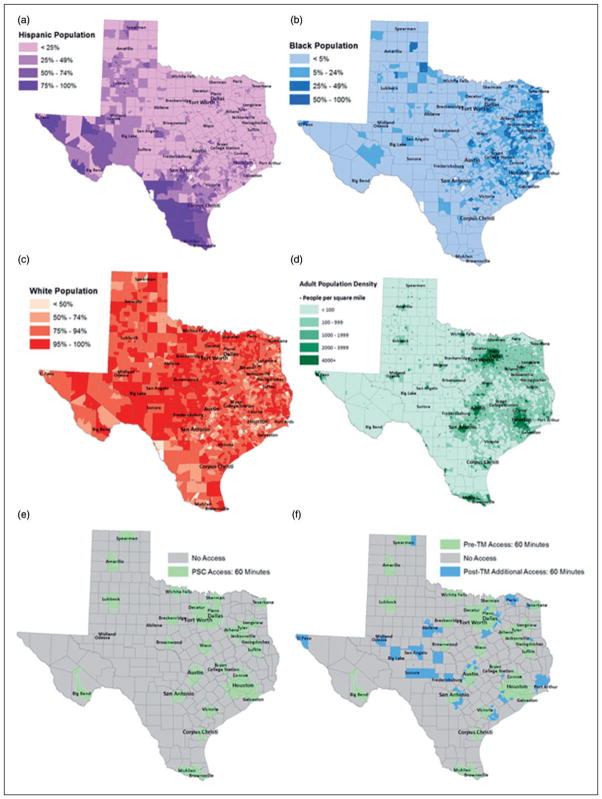
Racial and ethnic disparities have been previously reported in acute stroke care. We sought to determine the effect of telemedicine (TM) on access to acute stroke care for racial and ethnic minorities in the state of Texas. Data were collected from the US Census Bureau, The Joint Commission and the American Hospital Association. Access for racial and ethnic minorities was determined by summing the population that could reach a primary stroke centre (PSC) or telemedicine spoke within specified time intervals using validated models. TM extended access to stroke expertise by 1.5 million residents. The odds of providing 60-minute access via TM were similar in Blacks and Whites (prevalence odds ratios (POR) 1.000, 95% CI 1.000-1.000), even after adjustment for urbanization (POR 1.000, 95% CI 1.000-1.001). The odds of providing access via TM were also similar for Hispanics and non-Hispanics (POR 1.000, 95% CI 1.000-1.000), even after adjustment for urbanization (POR 1.000, 95% CI 1.000-1.000). We found that telemedicine increased access to acute stroke care for 1.5 million Texans. While racial and ethnic disparities exist in other components of stroke care, we did not find evidence of disparities in access to the acute stroke expertise afforded by telemedicine.
Keywords: Teleneurology; ethnic minorities; healthcare access; racial minorities; tele-stroke; telemedicine.
© The Author(s) 2015.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Towfighi A, Saver JL. Stroke declines from third to fourth leading cause of death in the United States: Historical perspective and challenges ahead. Stroke. 2011;42:2351–2355. - PubMed
-
- Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA stroke study group. N Engl J Med. 1995;333:1581–1587. - PubMed
-
- Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–1329. - PubMed
-
- Reeves MJ, Arora S, Broderick JP, et al. Acute stroke care in the US: Results from 4 pilot prototypes of the Paul Coverdell national acute stroke registry. Stroke. 2005;36:1232–1240. - PubMed
-
- Kleindorfer D, Lindsell CJ, Brass L, et al. National US estimates of recombinant tissue plasminogen activator use: ICD-9 codes substantially underestimate. Stroke. 2008;39:924–928. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
