

Significant Transplantation-Related Mortality from Respiratory Virus Infections within the First One Hundred Days in Children after Hematopoietic Stem Cell Transplantation
- PMID: 26117558
- PMCID: PMC7110880
- DOI: 10.1016/j.bbmt.2015.06.015
Significant Transplantation-Related Mortality from Respiratory Virus Infections within the First One Hundred Days in Children after Hematopoietic Stem Cell Transplantation
Abstract
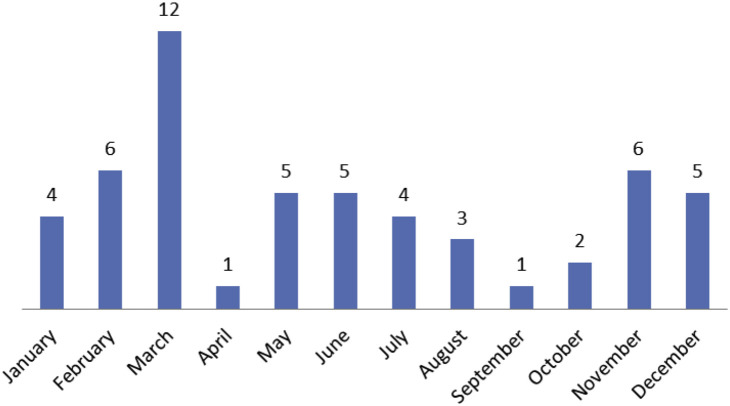
Respiratory viral infections (RVI) are important in hematopoietic stem cell transplantations (HSCT) and knowledge regarding incidence, morbidity, mortality, and long-term pulmonary complications is limited. We report a study to evaluate incidence and outcomes, both short and long-term, of RVI in children receiving HSCT. Between January 2000 and December 2012, 844 patients underwent hematopoietic stem cell transplantation (HSCT) at the Hospital for Sick Children: 491 were allogeneic and 353 were autologous. When screening for causes of death in the first year after HSCT in the 844 patients, we found that RVI as a cause of death was only evident in the first 100 days after HSCT. Fifty-four (6.5%) patients were found to have an RVI within the first 100 days after HSCT (allogeneic = 32, autologous = 22). Upper and lower respiratory tract infections were documented in 31 (57%) and 23 (43%) patients, respectively. Viruses were parainfluenza (35%), respiratory syncytial virus (28%), influenza (22%), adenovirus (7%), human metapneumovirus (4%), coronavirus (2%), and rhinovirus (2%). Three patients relapsed with their primary disease before day 100 and were excluded. The overall mortality for the remaining 51 patients was 10% (allogeneic = 4, autologous = 1). All 5 deaths were directly attributable to RVI and all 5 deaths occurred in patients with a lower respiratory tract infection. The remaining patients were followed for a median of 4.3 years (range, 1.4 to 11.8) and no chronic pulmonary complications were observed. A clear seasonal pattern for contracting RVI was evident with 65% of total RVI occurring between October and March (35 of 427 versus 19 of 417, P = .03). Given the significant mortality from RVI and the challenges in preventing them, choosing the time to start HSCT, whenever possible, may help prevent RVI and improve outcomes.
Keywords: Children; Hematopoietic stem cell transplantation; Mortality; Respiratory virus infection.
Copyright © 2015 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Kim Y.J., Boeckh M., Englund J.A. Community respiratory virus infections in immunocompromised patients: hematopoietic stem cell and solid organ transplant recipients, and individuals with human immunodeficiency virus infection. Semin Respir Crit Care Med. 2007;28:222–242. - PubMed
-
- Ison M.G., Hayden F.G. Viral infections in immunocompromised patients: what's new with respiratory viruses? Curr Opin Infect Dis. 2002;15:355–367. - PubMed
-
- Ljungman P., Ward K.N., Crooks B.N. Respiratory virus infections after stem cell transplantation: a prospective study from the Infectious Diseases Working Party of the European Group for Blood and Marrow Transplantation. Bone Marrow Transplant. 2001;28:479–484. - PubMed
-
- Kontoyiannis D.P., Lewis R.E., Marr K. The burden of bacterial and viral infections in hematopoietic stem cell transplant. Biol Blood Marrow Transplant. 2009;15(1 Suppl):128–133. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
