

An Economic Evaluation of Home Versus Laboratory-Based Diagnosis of Obstructive Sleep Apnea
- PMID: 26118558
- PMCID: PMC4481018
- DOI: 10.5665/sleep.4804
An Economic Evaluation of Home Versus Laboratory-Based Diagnosis of Obstructive Sleep Apnea
Abstract
Study objectives: We conducted an economic analysis of the HomePAP study, a multicenter randomized clinical trial that compared home-based versus laboratory-based testing for the diagnosis and management of obstructive sleep apnea (OSA).
Design: A cost-minimization analysis from the payer and provider perspectives was performed, given that 3-mo clinical outcomes were equivalent.
Setting: Seven academic sleep centers.
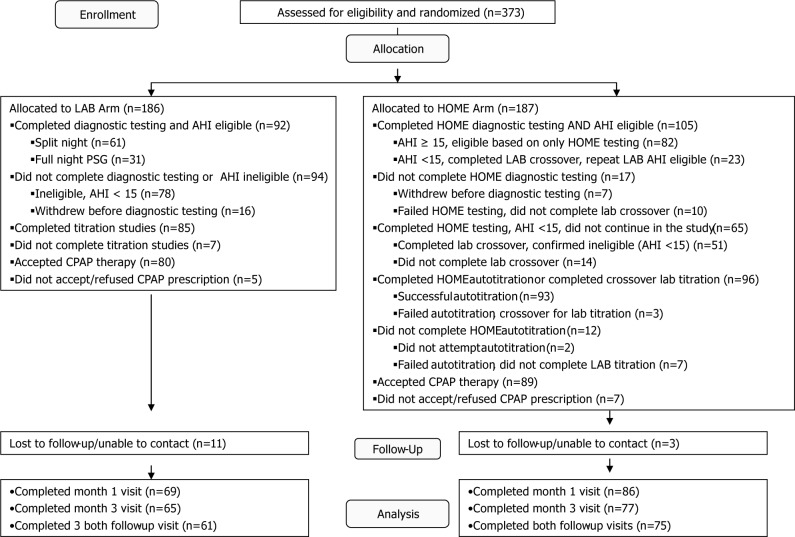
Participants: There were 373 subjects at high risk for moderate to severe OSA.
Interventions: Subjects were randomized to either home-based limited channel portable monitoring followed by unattended autotitration with continuous positive airway pressure (CPAP), versus a traditional pathway of in-laboratory sleep study and CPAP titration.
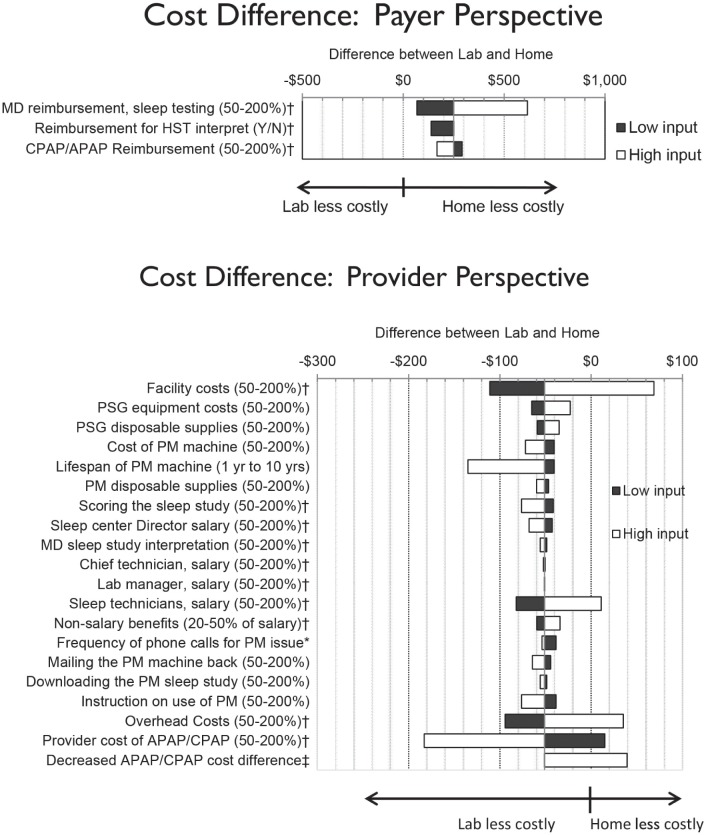
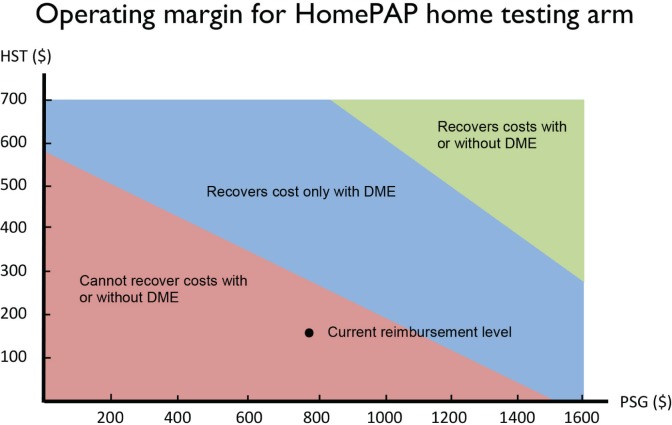
Measurements and results: From the payer perspective, per subject costs for the laboratory-based pathway were $1,840 (95% confidence interval [CI] $1,660, $2,015) compared to $1,575 (95% CI $1,439, $1,716) for the home-based pathway under the base case. Costs were $264 (95% CI $39, $496, P = 0.02) in favor of the home arm. From the provider perspective, per subject costs for the laboratory arm were $1,697 (95% CI $1,566, $1,826) compared to $1,736 (95% CI $1,621, $1,857) in the home arm, for a difference of $40 (95% CI -$213, $142, P = 0.66) in favor of the laboratory arm under the base case. The provider operating margin was $142 (95% CI $85, $202,P < 0.01) in the laboratory arm, compared to a loss of -$161 (95% CI -$202, -$120, P < 0.01) in the home arm.
Conclusions: For payers, a home-based diagnostic pathway for obstructive sleep apnea with robust patient support incurs fewer costs than a laboratory-based pathway. For providers, costs are comparable if not higher, resulting in a negative operating margin.
Clinicaltrialsgov identifier: NCT00642486.
Keywords: cost effectiveness analysis; cost minimization analysis; home sleep testing; obstructive sleep apnea; operating margin; out-of-center testing; portable monitor; sleep medicine.
© 2015 Associated Professional Sleep Societies, LLC.
Figures
References
-
- Mulgrew AT, Fox N, Ayas NT, Ryan CF. Diagnosis and initial management of obstructive sleep apnea without polysomnography: a randomized validation study. Ann Intern Med. 2007;146:157–66. - PubMed
-
- Antic NA, Buchan C, Esterman A, et al. A randomized controlled trial of nurse-led care for symptomatic moderate-severe obstructive sleep apnea. Am J Respir Crit Care Med. 2009;179:501–8. - PubMed
-
- Kuna ST, Gurubhagavatula I, Maislin G, et al. Noninferiority of functional outcome in ambulatory management of obstructive sleep apnea. Am J Respir Crit Care Med. 2011;183:1238–44. - PubMed
-
- Skomro RP, Gjevre J, Reid J, et al. Outcomes of home-based diagnosis and treatment of obstructive sleep apnea. Chest. 2010;138:257–63. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
