

Cost-Effectiveness Analysis of a Capitated Patient Navigation Program for Medicare Beneficiaries with Lung Cancer
- PMID: 26119569
- PMCID: PMC4799903
- DOI: 10.1111/1475-6773.12333
Cost-Effectiveness Analysis of a Capitated Patient Navigation Program for Medicare Beneficiaries with Lung Cancer
Abstract
Objective: To assess the cost-effectiveness of implementing a patient navigation (PN) program with capitated payment for Medicare beneficiaries diagnosed with lung cancer.
Data sources/study setting: Cost-effectiveness analysis.
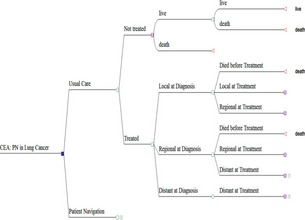
Study design: A Markov model to capture the disease progression of lung cancer and characterize clinical benefits of PN services as timeliness of treatment and care coordination. Taking a payer's perspective, we estimated the lifetime costs, life years (LYs), and quality-adjusted life years (QALYs) and addressed uncertainties in one-way and probabilistic sensitivity analyses.
Data collection/extraction methods: Model inputs were extracted from the literature, supplemented with data from a Centers for Medicare and Medicaid Services demonstration project.
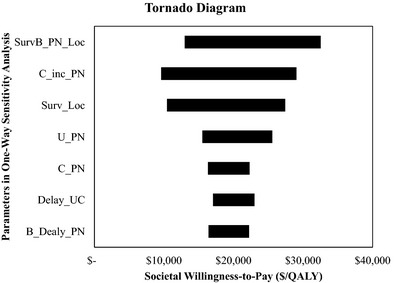
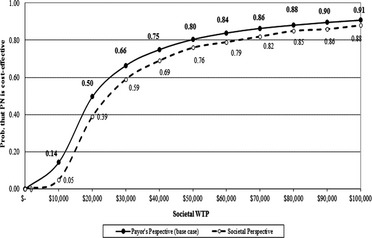
Principal findings: Compared to usual care, PN services incurred higher costs but also yielded better outcomes. The incremental cost and effectiveness was $9,145 and 0.47 QALYs, respectively, resulting in an incremental cost-effectiveness ratio of $19,312/QALY. One-way sensitivity analysis indicated that findings were most sensitive to a parameter capturing PN survival benefit for local-stage patients. CE-acceptability curve showed the probability that the PN program was cost-effective was 0.80 and 0.91 at a societal willingness-to-pay of $50,000 and $100,000/QALY, respectively.
Conclusion: Instituting a capitated PN program is cost-effective for lung cancer patients in Medicare. Future research should evaluate whether the same conclusion holds in other cancers.
Keywords: Cost-effectiveness analysis; lung cancer; patient navigation.
© Health Research and Educational Trust.
Figures
References
-
- ACS . 2013. American Cancer Society. Cancer Facts & Figures 2013. Atlanta, GA: American Cancer Society.
-
- Alsamarai, S. , Yao X., Cain H. C., Chang B. W., Chao H. H., Connery D. M., Deng Y., Garla V. N., Hunnibell L. S., Kim A. W., Obando J. A., Taylor C., Tellides G., and Rose M. G.. 2013. “The Effect of a Lung Cancer Care Coordination Program on Timeliness of Care.” Clinical Lung Cancer 14 (5): 527–534. - PubMed
-
- Bjegovich‐Weidman, M. , Haid M., Kumar S., Huibregtse C., McDonald J., and Krishnan S.. 2010. “Establishing a Community‐Based Lung Cancer Multidisciplinary Clinic as Part of a Large Integrated Health Care System: Aurora Health Care.” Journal of Oncology Practice/American Society of Clinical Oncology 6 (6): e27–e30. - PMC - PubMed
-
- Briggs, A. H. , Claxton K., and Sculpher M.. 2007. Decision Modelling for Health Economic Evaluation. New York: Oxford University Press.
-
- Davidoff, A. J. , Erten M., Shaffer T., Shoemaker J. S., Zuckerman I. H., Pandya N., Tai M. H., Ke X., and Stuart B.. 2013. “Out‐of‐Pocket Health Care Expenditure Burden for Medicare Beneficiaries with Cancer.” Cancer 119 (6): 1257–1265. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
