

A comparison of location of acute symptomatic vs. 'silent' small vessel lesions
- PMID: 26120782
- PMCID: PMC4737263
- DOI: 10.1111/ijs.12558
A comparison of location of acute symptomatic vs. 'silent' small vessel lesions
Abstract
Background: Acute lacunar ischaemic stroke, white matter hyperintensities, and lacunes are all features of cerebral small vessel disease. It is unclear why some small vessel disease lesions present with acute stroke symptoms, whereas others typically do not.
Aim: To test if lesion location could be one reason why some small vessel disease lesions present with acute stroke, whereas others accumulate covertly.
Methods: We identified prospectively patients who presented with acute lacunar stroke symptoms with a recent small subcortical infarct confirmed on magnetic resonance diffusion imaging. We compared the distribution of the acute infarcts with that of white matter hyperintensity and lacunes using computational image mapping methods.
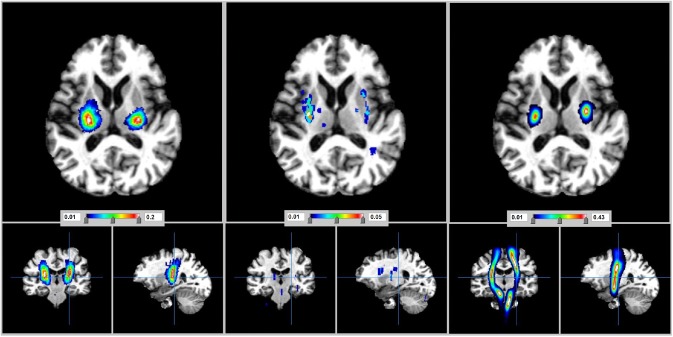
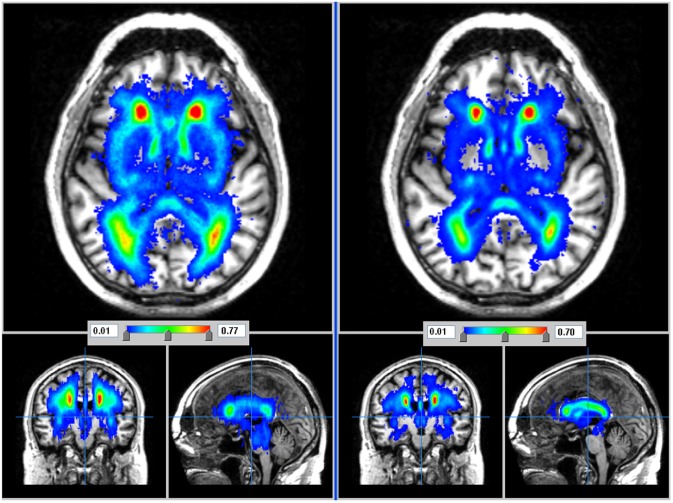
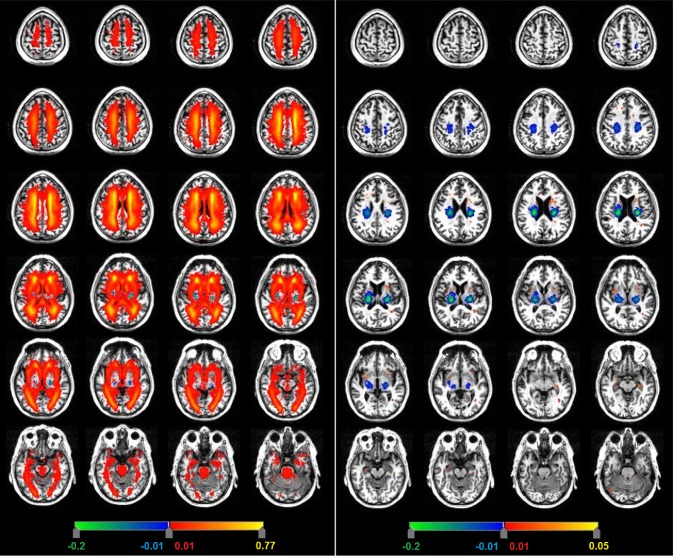
Results: In 188 patients, mean age 67 ± standard deviation 12 years, the lesions that presented with acute lacunar ischaemic stroke were located in or near the main motor and sensory tracts in (descending order): posterior limb of the internal capsule (probability density 0·2/mm(3)), centrum semiovale (probability density = 0·15/mm(3)), medial lentiform nucleus/lateral thalamus (probability density = 0·09/mm(3)), and pons (probability density = 0·02/mm(3)). Most lacunes were in the lentiform nucleus (probability density = 0·01-0·04/mm(3) ) or external capsule (probability density = 0·05/mm(3)). Most white matter hyperintensities were in centrum semiovale (except for the area affected by the acute symptomatic infarcts), external capsules, basal ganglia, and brainstem, with little overlap with the acute symptomatic infarcts (analysis of variance, P < 0·01).
Conclusions: Lesions that present with acute lacunar ischaemic stroke symptoms may be more likely noticed by the patient through affecting the main motor and sensory tracts, whereas white matter hyperintensity and asymptomatic lacunes mainly affect other areas. Brain location could at least partly explain the symptomatic vs. covert development of small vessel disease.
Keywords: acute lacunar infarct; lacunar stroke; lacunes; small vessel disease; stroke; white matter hyperintensities.
© 2015 The Authors. International Journal of Stroke published by John Wiley & Sons Ltd on behalf of World Stroke Organization.
Figures
References
-
- Sacco S, Marini C, Totaro R, Russo T, Cerone D, Carolei A. A population‐based study of the incidence and prognosis of lacunar stroke. Neurology 2006; 66:1335–1338. - PubMed
-
- Potter GM, Doubal FN, Jackson CA et al Counting cavitating lacunes underestimates the burden of lacunar infarction. Stroke 2010; 41:267–272. - PubMed
-
- Loos CM, Staals J, Wardlaw JM, van Oostenbrugge RJ. Cavitation of deep lacunar infarcts in patients with first‐ever lacunar stroke: a 2‐year follow‐up study with MR. Stroke 2012; 43:2245–2247. - PubMed
-
- Moreau F, Patel S, Lauzon ML et al Cavitation after acute symptomatic lacunar stroke depends on time, location, and MRI sequence. Stroke 2012; 43:1837–1842. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
