

The Impact of Timing of Antibiotics on Outcomes in Severe Sepsis and Septic Shock: A Systematic Review and Meta-Analysis
- PMID: 26121073
- PMCID: PMC4597314
- DOI: 10.1097/CCM.0000000000001142
The Impact of Timing of Antibiotics on Outcomes in Severe Sepsis and Septic Shock: A Systematic Review and Meta-Analysis
Abstract
Objectives: We sought to systematically review and meta-analyze the available data on the association between timing of antibiotic administration and mortality in severe sepsis and septic shock.
Data sources: A comprehensive search criteria was performed using a predefined protocol.
Inclusion criteria: adult patients with severe sepsis or septic shock, reported time to antibiotic administration in relation to emergency department triage and/or shock recognition, and mortality.
Exclusion criteria: immunosuppressed populations, review article, editorial, or nonhuman studies.
Data extraction: Two reviewers screened abstracts with a third reviewer arbitrating. The effect of time to antibiotic administration on mortality was based on current guideline recommendations: 1) administration within 3 hours of emergency department triage and 2) administration within 1 hour of severe sepsis/septic shock recognition. Odds ratios were calculated using a random effect model. The primary outcome was mortality.
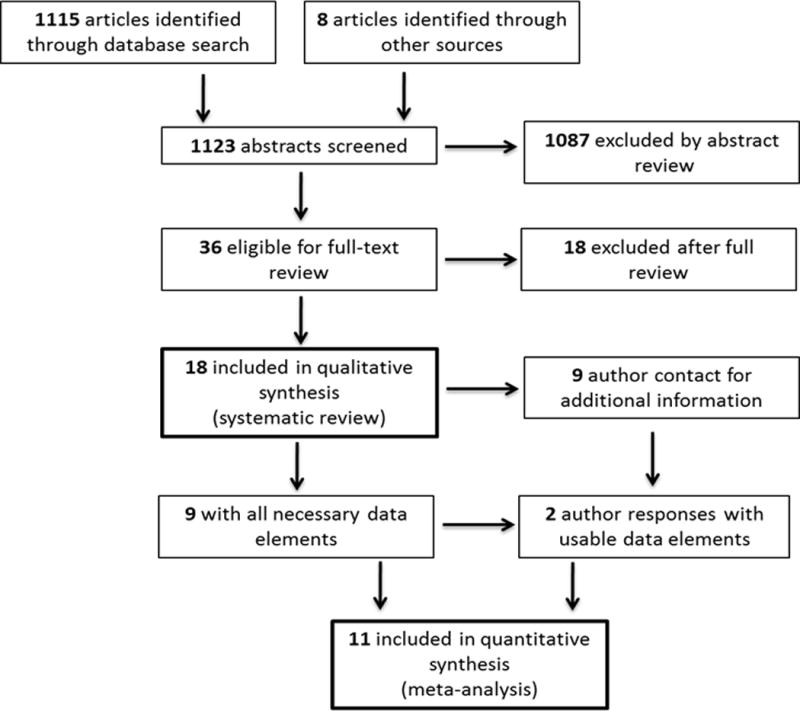
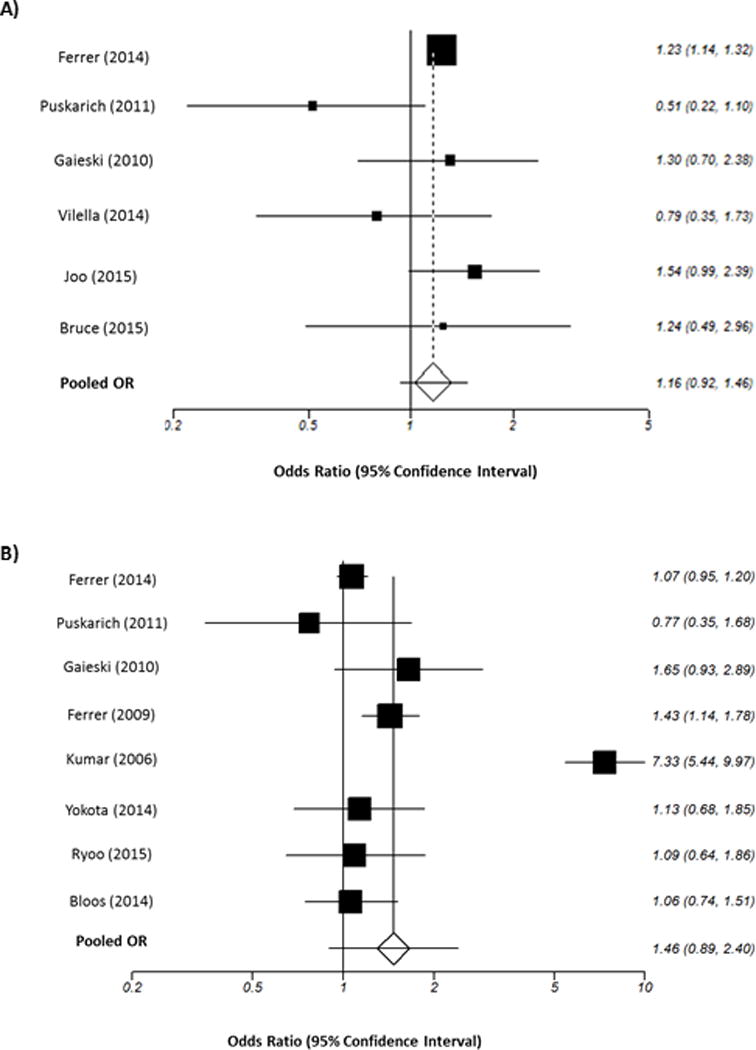
Data synthesis: A total of 1,123 publications were identified and 11 were included in the analysis. Among the 11 included studies, 16,178 patients were evaluable for antibiotic administration from emergency department triage. Patients who received antibiotics more than 3 hours after emergency department triage (< 3 hr reference) had a pooled odds ratio for mortality of 1.16 (0.92-1.46; p = 0.21). A total of 11,017 patients were evaluable for antibiotic administration from severe sepsis/septic shock recognition. Patients who received antibiotics more than 1 hour after severe sepsis/shock recognition (< 1 hr reference) had a pooled odds ratio for mortality of 1.46 (0.89-2.40; p = 0.13). There was no increased mortality in the pooled odds ratios for each hourly delay from less than 1 to more than 5 hours in antibiotic administration from severe sepsis/shock recognition.
Conclusion: Using the available pooled data, we found no significant mortality benefit of administering antibiotics within 3 hours of emergency department triage or within 1 hour of shock recognition in severe sepsis and septic shock. These results suggest that currently recommended timing metrics as measures of quality of care are not supported by the available evidence.
Conflict of interest statement
The authors have no conflicts of interest to report
Figures
Comment in
-
Timing of Therapy in Sepsis: Are Early Antibiotics Important for Prognosis?Crit Care Med. 2015 Sep;43(9):2030-1. doi: 10.1097/CCM.0000000000001179. Crit Care Med. 2015. PMID: 26274712 No abstract available.
-
Meta-analysis based on limited data shows no evidence to support the guideline recommendation for early administration of antibiotics in severe sepsis and septic shock.Evid Based Med. 2015 Dec;20(6):214-5. doi: 10.1136/ebmed-2015-110269. Epub 2015 Oct 12. Evid Based Med. 2015. PMID: 26459374 No abstract available.
-
Timing of Appropriate Antibiotics in Sepsis: How Much Does Each Hour Matter?Crit Care Med. 2016 Feb;44(2):e109-10. doi: 10.1097/CCM.0000000000001449. Crit Care Med. 2016. PMID: 26771802 No abstract available.
-
The authors reply.Crit Care Med. 2016 Feb;44(2):e110. doi: 10.1097/CCM.0000000000001513. Crit Care Med. 2016. PMID: 26771803 Free PMC article. No abstract available.
-
Systematic Bias in Meta-Analyses of Time to Antimicrobial in Sepsis Studies.Crit Care Med. 2016 Apr;44(4):e234-5. doi: 10.1097/CCM.0000000000001512. Crit Care Med. 2016. PMID: 26974458 No abstract available.
-
The authors reply.Crit Care Med. 2016 Apr;44(4):e235-6. doi: 10.1097/CCM.0000000000001550. Crit Care Med. 2016. PMID: 26974459 Free PMC article. No abstract available.
-
Time for a Randomized Controlled Trial to Investigate Optimal Time to Antibiotics for Patients With Sepsis.Crit Care Med. 2016 Apr;44(4):e236-7. doi: 10.1097/CCM.0000000000001514. Crit Care Med. 2016. PMID: 26974460 No abstract available.
-
The authors reply.Crit Care Med. 2016 Apr;44(4):e237. doi: 10.1097/CCM.0000000000001546. Crit Care Med. 2016. PMID: 26974461 Free PMC article. No abstract available.
-
Timing of Antibiotic Administration in Sepsis and Septic Shock: The Impact That a Meta-Analysis Does Not Depict.Crit Care Med. 2016 Oct;44(10):e1004. doi: 10.1097/CCM.0000000000001891. Crit Care Med. 2016. PMID: 27635498 No abstract available.
-
The authors reply.Crit Care Med. 2016 Oct;44(10):e1004-5. doi: 10.1097/CCM.0000000000001978. Crit Care Med. 2016. PMID: 27635499 Free PMC article. No abstract available.
-
Time Matters: Antibiotic Timing in Sepsis and Septic Shock.Crit Care Med. 2016 Oct;44(10):e1016-7. doi: 10.1097/CCM.0000000000001968. Crit Care Med. 2016. PMID: 27635516 No abstract available.
-
The authors reply.Crit Care Med. 2016 Oct;44(10):e1017-8. doi: 10.1097/CCM.0000000000002038. Crit Care Med. 2016. PMID: 27635517 Free PMC article. No abstract available.
-
Meta-Analysis of Time to Antimicrobial Therapy in Sepsis: Confounding as Well as Bias.Crit Care Med. 2017 Feb;45(2):e242-e243. doi: 10.1097/CCM.0000000000002162. Crit Care Med. 2017. PMID: 28098654 No abstract available.
-
The authors reply.Crit Care Med. 2017 Feb;45(2):e243-e244. doi: 10.1097/CCM.0000000000002178. Crit Care Med. 2017. PMID: 28098655 Free PMC article. No abstract available.
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001 Jul;29(7):1303–10. - PubMed
-
- Wang HE, Shapiro NI, Angus DC, Yealy DM. National estimates of severe sepsis in United States emergency departments. Crit Care Med. 2007 Aug;35(8):1928–36. - PubMed
-
- Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001 Nov 8;345(19):1368–77. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
