

High BRAF Mutation Frequency and Marked Survival Differences in Subgroups According to KRAS/BRAF Mutation Status and Tumor Tissue Availability in a Prospective Population-Based Metastatic Colorectal Cancer Cohort
- PMID: 26121270
- PMCID: PMC4484806
- DOI: 10.1371/journal.pone.0131046
High BRAF Mutation Frequency and Marked Survival Differences in Subgroups According to KRAS/BRAF Mutation Status and Tumor Tissue Availability in a Prospective Population-Based Metastatic Colorectal Cancer Cohort
Abstract
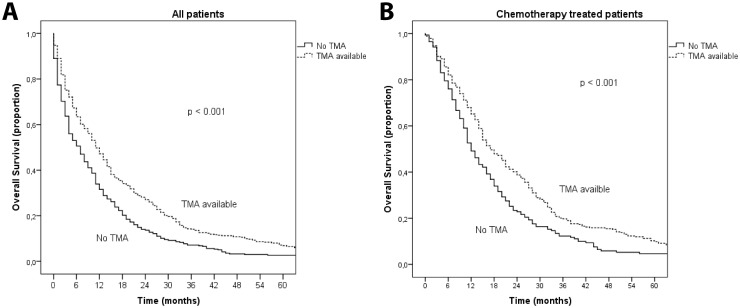
RAS and BRAF mutations impact treatment and prognosis of metastatic colorectal cancer patients (mCRC), but the knowledge is based on trial patients usually not representative for the general cancer population. Patient characteristics, treatment and efficacy according to KRAS, BRAF and MSI status were analyzed in a prospectively collected unselected population-based cohort of 798 non-resectable mCRC patients. The cohort contained many patients with poor performance status (39% PS 2-4) and elderly (37% age>75), groups usually not included in clinical trials. Patients without available tissue micro array (TMA) (42%) had worse prognostic factors and inferior survival (all patients; 7m vs 11m, chemotherapy-treated;12m vs 17m). The 92 patients (21%) with BRAF mutation had a poor prognosis regardless of microsatellite instability, but receipt of 1-2nd chemotherapy was similar to wildtype BRAF patients. Median survival in this cohort varied from 1 month in BRAF mutated patients not given chemotherapy to 26 months in wildtype KRAS/BRAF patients <75 years in good PS. TMA availability, BRAF mutation and KRAS mutation were all independent prognostic factors for survival. The observed 21% BRAF mutation incidence is higher than the previously and repeatedly reported incidence of 5-12% in mCRC. Screening for BRAF mutations before selection of treatment is relevant for many patients, especially outside clinical trials. A BRAF mutation only partly explained the very poor prognosis of many mCRC patients. Survival in unselected metastatic colorectal cancer patients is extremely variable and subgroups have an extremely short survival compared to trial patients. Patients without available TMA had worse prognostic factors and shorter survival, which questions the total generalizability of present TMA studies and implies that we lack information on the biologically worst mCRC cases. Lack of available tissue is an important underexposed issue which introduces sample bias, and this should be recognized more clearly when conclusions are made from translational mCRC studies.
Conflict of interest statement
Figures


References
-
- Van Cutsem E, Köhne CH, Láng I, Folprecht G, Nowacki MP, Cascinu S, et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J Clin Oncol 2011;29: 2011–9. 10.1200/JCO.2010.33.5091 - DOI - PubMed
-
- Tveit KM, Guren T, Glimelius B, Pfeiffer P, Sorbye H, Pyrhonen S, et al. Phase III trial of cetuximab with continuous or intermittent fluorouracil, leucovorin, and oxaliplatin (Nordic FLOX) versus FLOX alone in first-line treatment of metastatic colorectal cancer: the NORDIC-VII study. J Clin Oncol 2012;30: 1755–62. 10.1200/JCO.2011.38.0915 - DOI - PubMed
-
- Schwartzberg LS, Rivera F, Karthaus M, Fasola G, Canon JL, Hecht JR,et al. PEAK: a randomized, multicenter phase II study of panitumumab plus modified fluorouracil, leucovorin, and oxaliplatin (mFOLFOX6) or bevacizumab plus mFOLFOX6 in patients with previously untreated, unresectable, wild-type KRAS exon 2 metastatic colorectal cancer. J Clin Oncol 2014;32: 2240–7. 10.1200/JCO.2013.53.2473 - DOI - PubMed
-
- Maughan TS, Adams RA, Smith CG, Meade AM, Seymour MT, Wilson RH, et al. Addition of cetuximab to oxaliplatin-based first-line combination chemotherapy for treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial. Lancet 2011;377: 2103–14. 10.1016/S0140-6736(11)60613-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
