

Prognostic significance of minimal residual disease in high risk B-ALL: a report from Children's Oncology Group study AALL0232
- PMID: 26124497
- PMCID: PMC4543229
- DOI: 10.1182/blood-2015-03-633685
Prognostic significance of minimal residual disease in high risk B-ALL: a report from Children's Oncology Group study AALL0232
Abstract
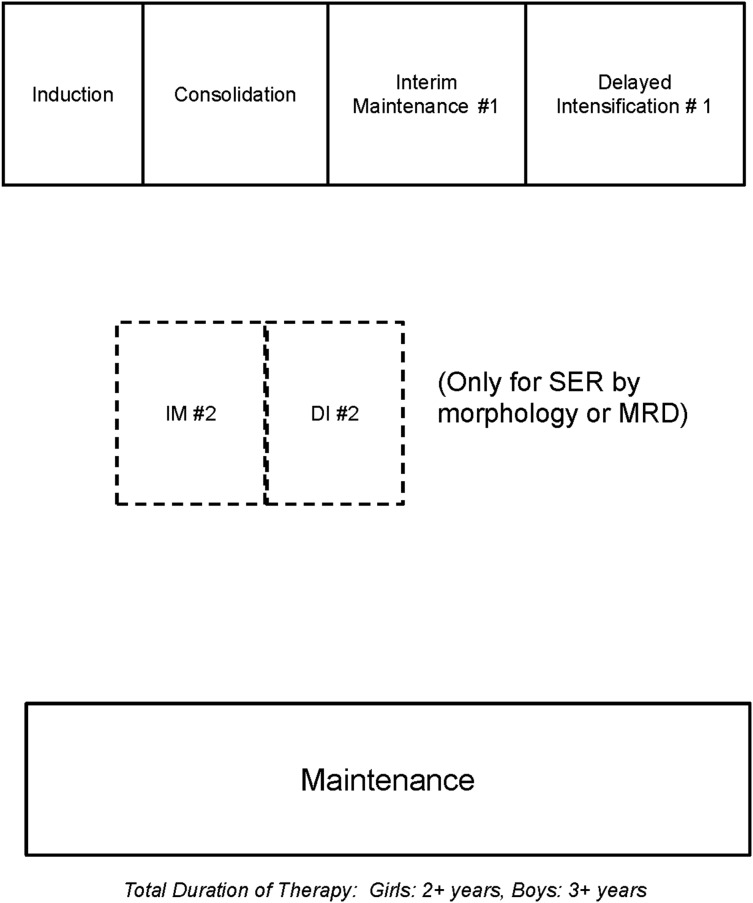
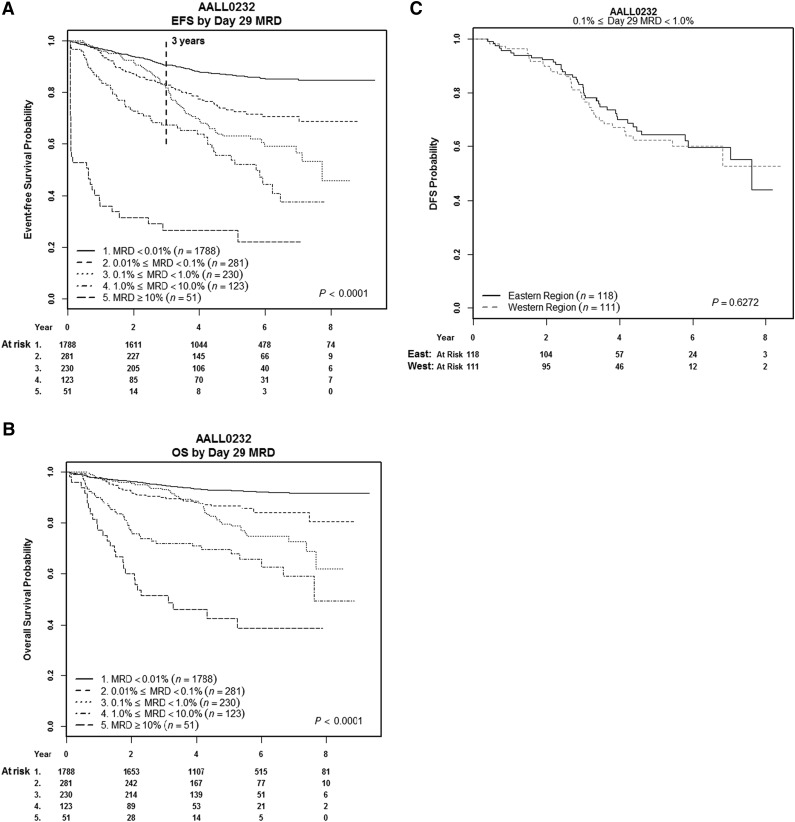
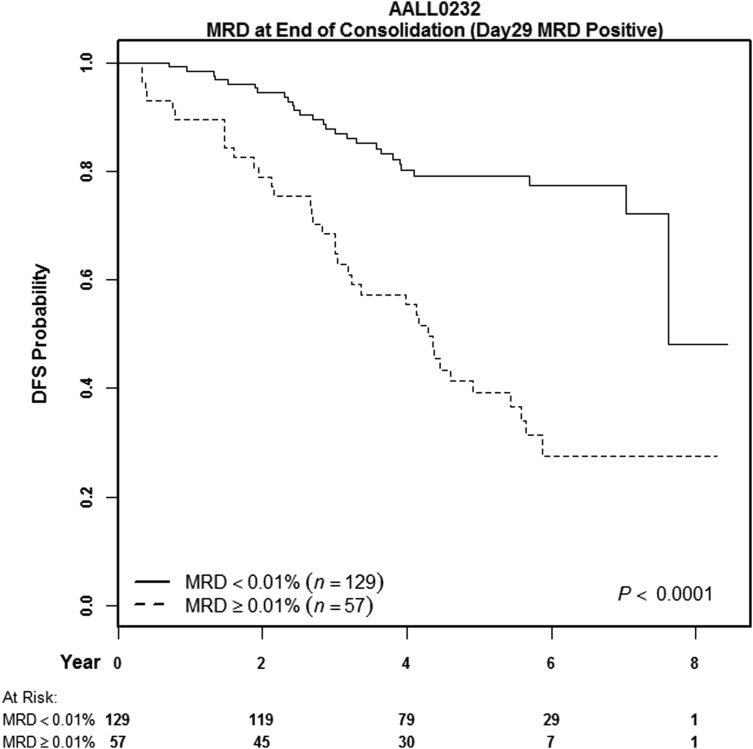
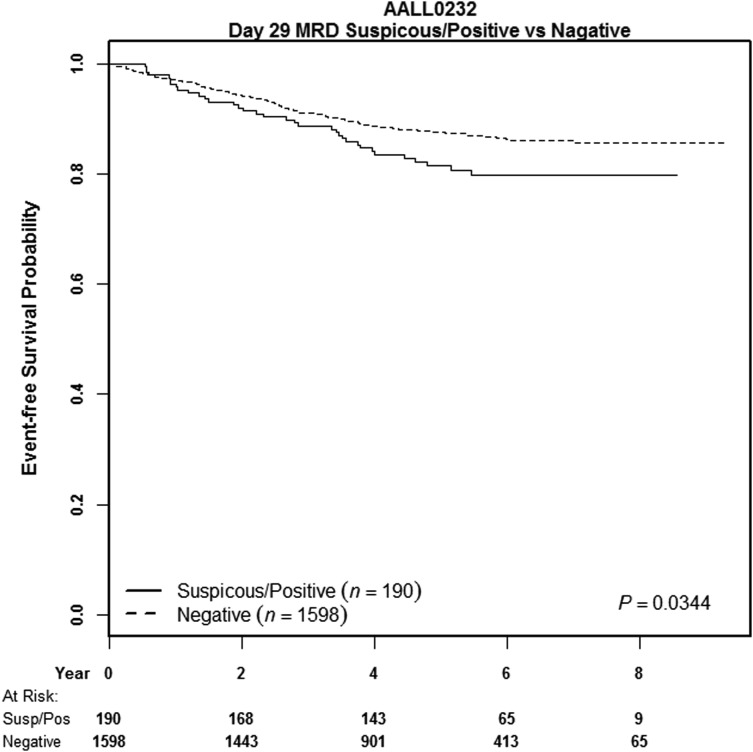
Minimal residual disease (MRD) is highly prognostic in pediatric B-precursor acute lymphoblastic leukemia (B-ALL). In Children's Oncology Group high-risk B-ALL study AALL0232, we investigated MRD in subjects randomized in a 2 × 2 factorial design to receive either high-dose methotrexate (HD-MTX) or Capizzi methotrexate (C-MTX) during interim maintenance (IM) or prednisone or dexamethasone during induction. Subjects with end-induction MRD ≥0.1% or those with morphologic slow early response were nonrandomly assigned to receive a second IM and delayed intensification phase. MRD was measured by 6-color flow cytometry in 1 of 2 reference labs, with excellent agreement between the two. Subjects with end-induction MRD <0.01% had a 5-year event-free survival (EFS) of 87% ± 1% vs 74% ± 4% for those with MRD 0.01% to 0.1%; increasing MRD amounts was associated with progressively worse outcome. Subjects converting from MRD positive to negative by end consolidation had a relatively favorable 79% ± 5% 5-year disease-free survival vs 39% ± 7% for those with MRD ≥0.01%. Although HD-MTX was superior to C-MTX, MRD retained prognostic significance in both groups (86% ± 2% vs 58% ± 4% for MRD-negative vs positive C-MTX subjects; 88% ± 2% vs 68% ± 4% for HD-MTX subjects). Intensified therapy given to subjects with MRD >0.1% did not improve either 5-year EFS or overall survival (OS). However, these subjects showed an early relapse rate similar to that seen in MRD-negative ones, with EFS/OS curves for patients with 0.1% to 1% MRD crossing those with 0.01% to 0.1% MRD at 3 and 4 years, thus suggesting that the intensified therapy altered the disease course of MRD-positive subjects. Additional interventions targeted at the MRD-positive group may further improve outcome. This trial was registered at www.clinicaltrials.gov as #NCT00075725.
Figures
References
-
- Cazzaniga G, Gaipa G, Rossi V, Biondi A. Minimal residual disease as a surrogate marker for risk assignment to ALL patients. Rev Clin Exp Hematol. 2003;7(3):292–323. - PubMed
-
- Conter V, Aricò M, Basso G, et al. Associazione Italiana di Ematologia ed Oncologia Pediatrica. Long-term results of the Italian Association of Pediatric Hematology and Oncology (AIEOP) Studies 82, 87, 88, 91 and 95 for childhood acute lymphoblastic leukemia. Leukemia. 2010;24(2):255–264. - PubMed
-
- Coustan-Smith E, Sancho J, Hancock ML, et al. Clinical importance of minimal residual disease in childhood acute lymphoblastic leukemia. Blood. 2000;96(8):2691–2696. - PubMed
-
- Dworzak MN, Fröschl G, Printz D, et al. Austrian Berlin-Frankfurt-Münster Study Group. Prognostic significance and modalities of flow cytometric minimal residual disease detection in childhood acute lymphoblastic leukemia. Blood. 2002;99(6):1952–1958. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
