

Effects of continuous fascia iliaca compartment blocks for postoperative analgesia in patients with hip fracture
- PMID: 26125194
- PMCID: PMC4532207
- DOI: 10.1155/2015/872651
Effects of continuous fascia iliaca compartment blocks for postoperative analgesia in patients with hip fracture
Abstract
Background: Effective analgesia is essential for the postoperative care of orthopedic patients.
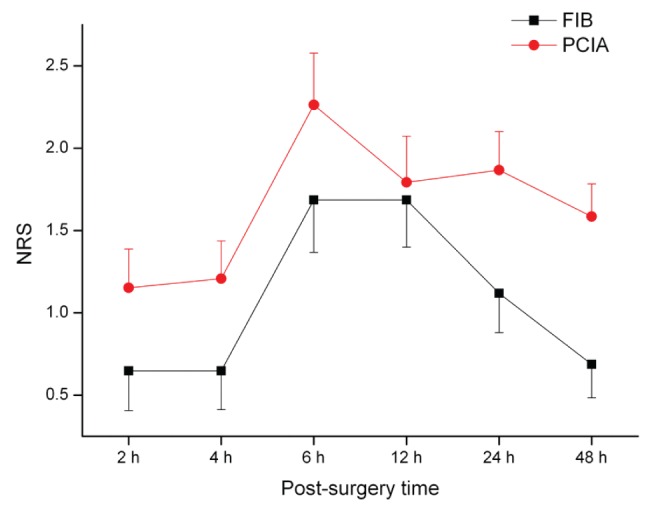
Objectives: To evaluate the efficacy of continuous fascia iliaca compartment block (FIB) as postoperative analgesia after hip fracture surgery, and to compare FIB with patient-controlled intravenous analgesia (PCIA) using fentanyl for 48 h postoperatively.
Methods: Patients with hip fractures who were scheduled for open reduction and internal fixation surgery using the antirotation proximal femoral nail technique were randomly assigned to the FIB or PCIA groups. Postoperative pain was assessed using a numeral rating scale at 2 h, 4 h, 6 h, 12 h, 24 h and 48 h after analgesia was started. Delirium, postoperative nausea and vomiting (PONV), and pruritus were also monitored.
Results: Patients in the FIB group reported less pain than those in the PCIA group (P=0.039, d=-0.3). The change in pain scores over time was similar between the two groups. There were six patients with PONV and five patients with pruritus in the PCIA group, while no PONV or pruritus was noticed in the FIB group (P=0.013). Ten (19.6%) patients in the FIB group and three (5.7%) patients in the PCIA group developed postoperative delirium (P=0.032, d=0.77).
Conclusion: Continuous FIB is a safe and effective technique for postoperative analgesia after hip fracture surgery, making it an option for pain management in elderly patients with hip fractures.
HISTORIQUE :: Il est essentiel d’assurer une analgésie efficace en orthopédie postopératoire.
OBJECTIFS :: Évaluer l’efficacité du bloc du compartiment ilio-fascial (BCIF) continu en analgésie postopératoire après une chirurgie pour fracture de la hanche, et comparer le BCIF à l’analgésie intraveineuse contrôlée par le patient (AICP) au fentanyl pendant les 48 heures suivant l’opération.
MÉTHODOLOGIE :: Les patients ayant une facture de la hanche qui devaient subir une chirurgie ouverte de réduction et de fixation interne par la technique du clou antirotation pour fracture du fémur proximal ont été répartis au hasard entre le groupe de BCIF et d’AICP. La douleur postopératoire a été évaluée au moyen d’une échelle d’évaluation numérique deux, quatre, six, 12, 24 et 48 heures après le début de l’analgésie. Le délire, les nausées postopératoires et les vomissements (NPOV) ainsi que le prurit ont également été surveillés.
RÉSULTATS :: Les patients du groupe du BCIF ont déclaré souffrir moins que ceux du groupe d’AICP (P=0,039, d=−0,3). Le changement dans les scores de douleur au fil du temps était similaire dans les deux groupes. Six patients souffraient de NPOV et cinq, de prurit dans le groupe d’AICP, mais aucun cas de NPOV ni de prurit n’a été observé dans le groupe de BCIF (P=0,013). Dix patients (19,6 %) du groupe de BCIF et trois (5,7 %) du groupe d’AICP ont souffert de délire postopératoire (P=0,032, d=0,77).
CONCLUSION :: Le BCIF continu est une technique d’analgésie postopératoire sécuritaire et efficace après une chirurgie pour fracture de la hanche, qui peut être utilisée pour gérer la douleur chez les patients âgés ayant une telle fracture.
Figures
References
-
- Ekstein, Weinbroum AA. Immediate postoperative pain in orthopedic patients is more intense and requires more analgesia than in post-laparotomy patients. Pain Med. 2010;12:308–13. - PubMed
-
- Liu SS, Wu CL. The effect of analgesic technique on postoperative patient-reported outcomes including analgesia: A systematic review. Anesth Analg. 2007;105:789–808. - PubMed
-
- Morau D, Lopez S, Biboulet P, Bernard N, Amar J, Capdevila X. Comparison of continuous 3-in-1 and fascia iliaca compartment blocks for postoperative analgesia: Feasibility, catheter migration, distribution of sensory block, and analgesic efficacy. Reg Anesth Pain Med. 2003;28:309–14. - PubMed
-
- Foss NB, Kristensen BB, Bundgaard M, et al. Fascia iliaca compartment blockade for acute pain control in hip fracture patients: A randomized, placebo-controlled trial. Anesthesiology. 2007;106:773–8. - PubMed
-
- Singelyn FJ, Deyaert M, Joris D, Pendeville E, Gouverneur JM. Effects of intravenous patient-controlled analgesia with morphine, continuous epidural analgesia, and continuous three-in-one block on postoperative pain and knee rehabilitation after unilateral total knee arthroplasty. Anesth Analg. 1998;87:88–92. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
