

Provider Attitudes and Screening Practices Following Changes in Breast and Cervical Cancer Screening Guidelines
- PMID: 26129780
- PMCID: PMC4700005
- DOI: 10.1007/s11606-015-3449-5
Provider Attitudes and Screening Practices Following Changes in Breast and Cervical Cancer Screening Guidelines
Abstract
Background: Changes to national guidelines for breast and cervical cancer screening have created confusion and controversy for women and their primary care providers.
Objective: To characterize women's primary health care provider attitudes towards screening and changes in practice in response to recent revisions in guidelines for breast and cervical cancer screening.
Design, setting, participants: In 2014, we distributed a confidential web and mail survey to 668 women's health care providers affiliated with the four clinical care networks participating in the three PROSPR (Population-based Research Optimizing Screening through Personalized Regimens) consortium breast cancer research centers (385 respondents; response rate 57.6 %).
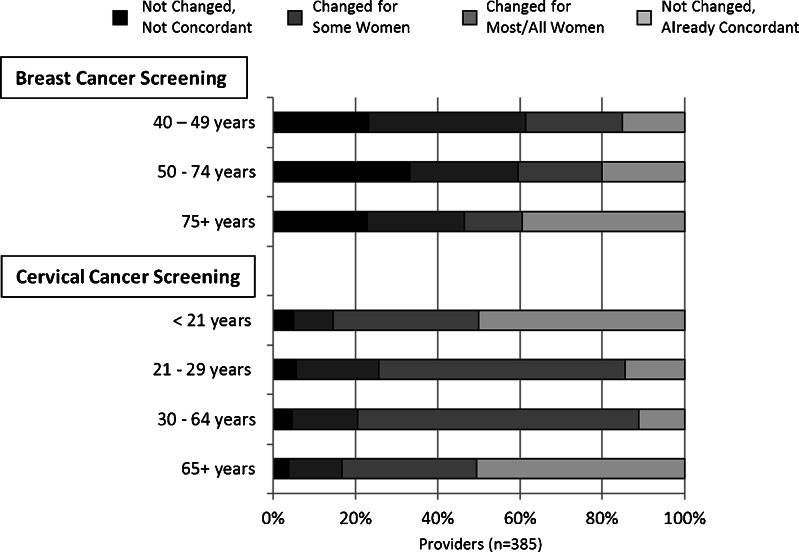
Main measures: We assessed self-reported attitudes toward breast and cervical cancer screening, as well as practice changes in response to the most recent revisions of the U.S. Preventive Services Task Force (USPSTF) recommendations.
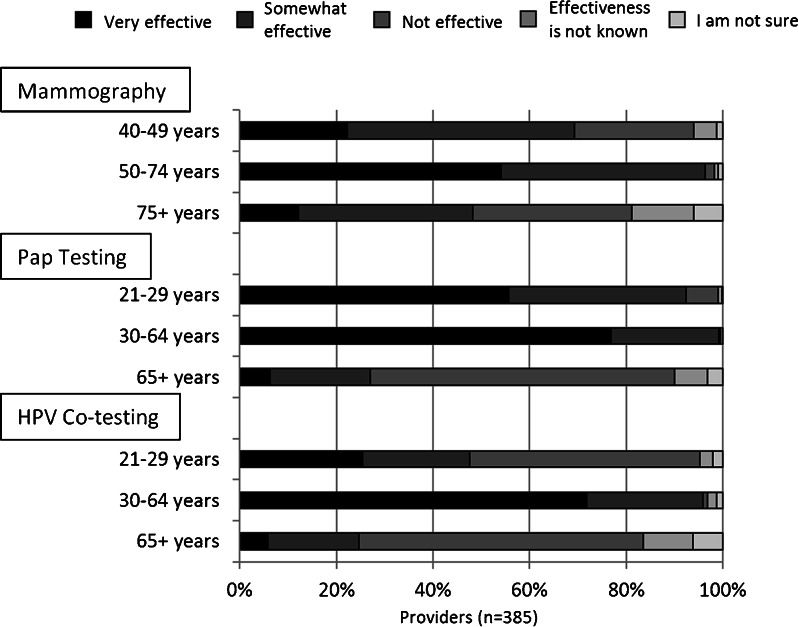
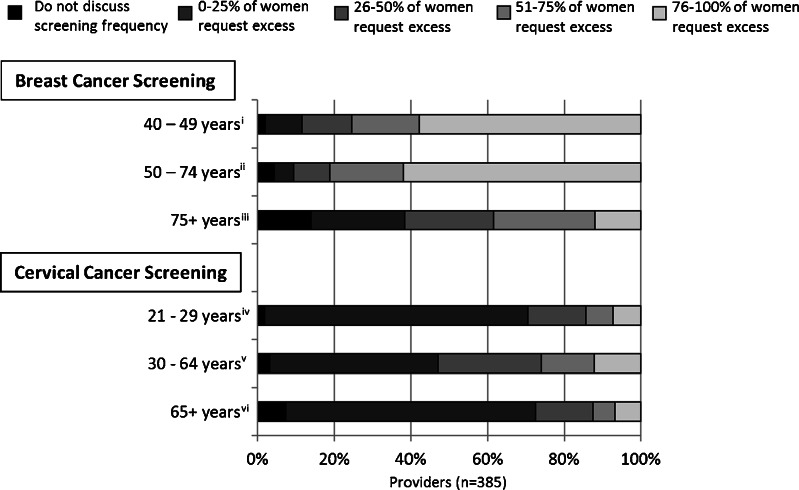
Key results: The majority of providers believed that mammography screening was effective for reducing cancer mortality among women ages 40-74 years, and that Papanicolaou (Pap) testing was very effective for women ages 21-64 years. While the USPSTF breast and cervical cancer screening recommendations were widely perceived by the respondents as influential, 75.7 and 41.2 % of providers (for mammography and cervical cancer screening, respectively) reported screening practices in excess of those recommended by USPSTF. Provider-reported barriers to concordance with guideline recommendations included: patient concerns (74 and 36 % for breast and cervical, respectively), provider disagreement with the recommendations (50 and 14 %), health system measurement of a provider's screening practices that use conflicting measurement criteria (40 and 21 %), concern about malpractice risk (33 and 11 %), and lack of time to discuss the benefits and harms with their patients (17 and 8 %).
Conclusions: Primary care providers do not consistently follow recent USPSTF breast and cervical cancer screening recommendations, despite noting that these guidelines are influential.
Keywords: breast cancer screening; cervical cancer screening; clinical practice guidelines; primary care; provider practice patterns.
Figures
Comment in
-
Capsule Commentary on Haas et al., Provider Attitudes and Screening Practices Following Changes in Breast and Cervical Cancer Screening Guidelines.J Gen Intern Med. 2016 Jan;31(1):103. doi: 10.1007/s11606-015-3490-4. J Gen Intern Med. 2016. PMID: 26259763 Free PMC article. No abstract available.
References
-
- Feldman S. Can the new cervical cancer screening and management guidelines be simplified? JAMA Intern Med. 2014. - PubMed
-
- Screening for breast cancer: U.S. Preventive services task force recommendation statement. Ann Intern Med 2009;151:716–726, W-236. - PubMed
-
- Mandelblatt JS, Cronin KA, Bailey S, Berry DA, de Koning HJ, Draisma G, Huang H, Lee SJ, Munsell M, Plevritis SK, Ravdin P, Schechter CB, Sigal B, Stoto MA, Stout NK, van Ravesteyn NT, Venier J, Zelen M, Feuer EJ. Effects of mammography screening under different screening schedules: model estimates of potential benefits and harms. Ann Intern Med. 2009;151:738–47. doi: 10.7326/0003-4819-151-10-200911170-00010. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
