

Prognostic Importance of Impaired Systolic Function in Heart Failure With Preserved Ejection Fraction and the Impact of Spironolactone
- PMID: 26130119
- PMCID: PMC4526442
- DOI: 10.1161/CIRCULATIONAHA.115.015884
Prognostic Importance of Impaired Systolic Function in Heart Failure With Preserved Ejection Fraction and the Impact of Spironolactone
Abstract
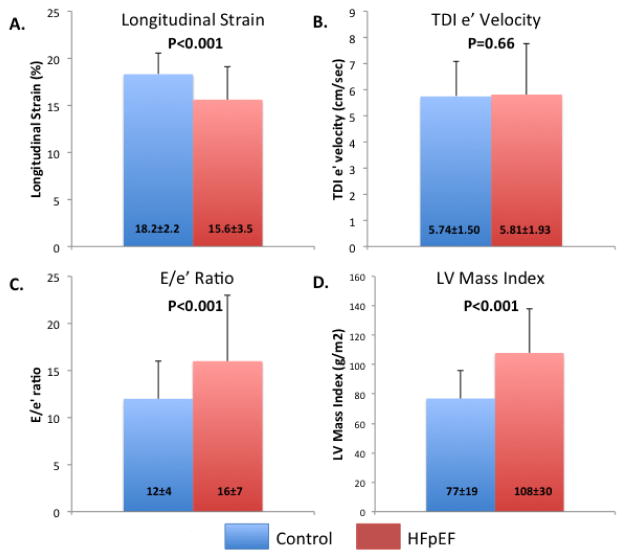
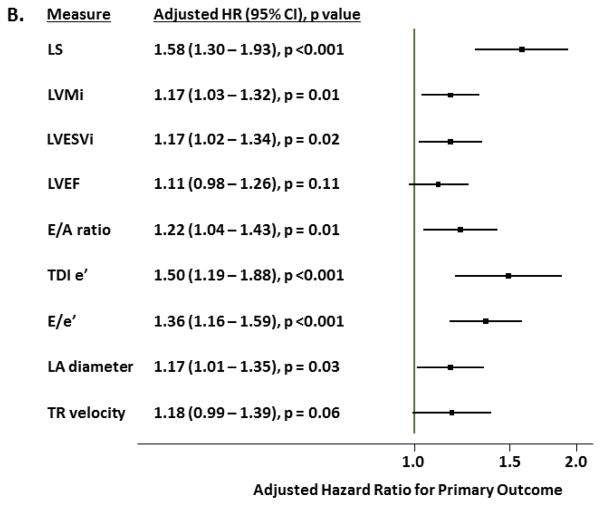
Background: Impairment in left ventricular systolic function has been described in heart failure (HF) with preserved ejection fraction (HFpEF), but its prognostic relevance is not known. We determined whether left ventricular longitudinal strain (LS) is predictive of cardiovascular outcomes in HFpEF beyond clinical and conventional echocardiographic measures.
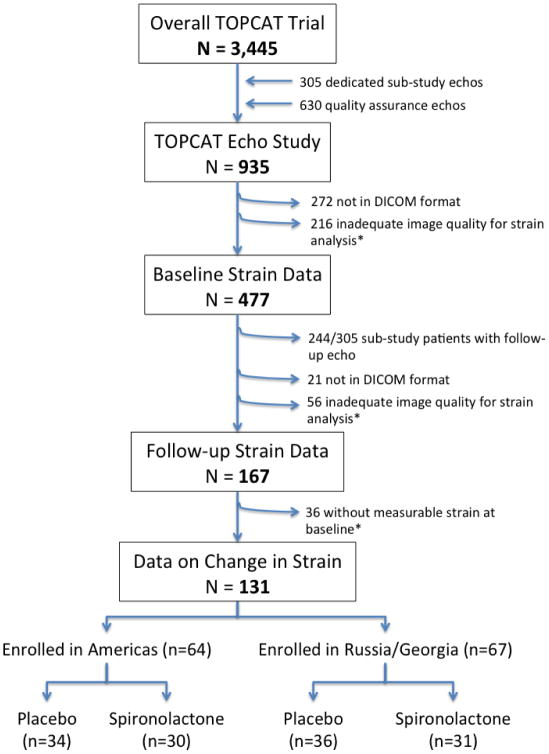
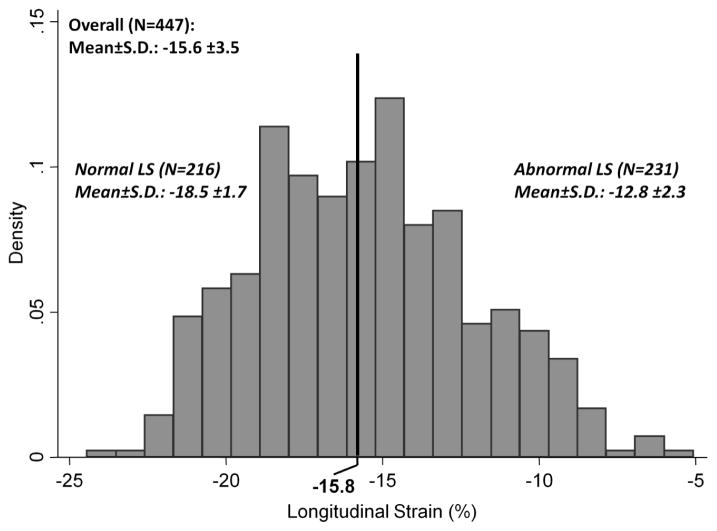
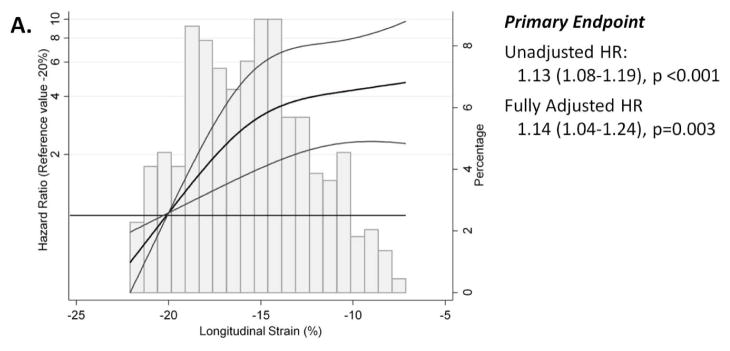
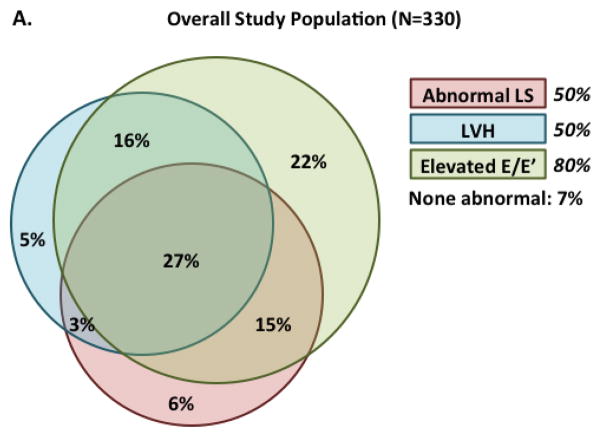
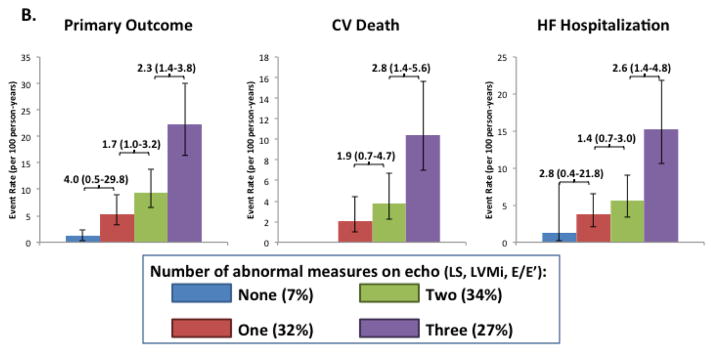
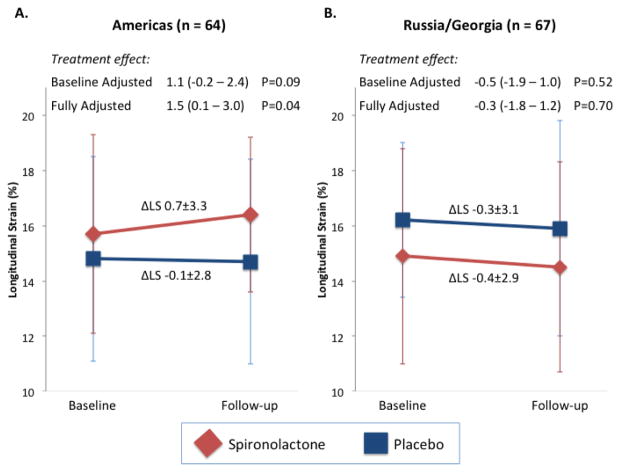
Methods and results: LS was assessed by 2-dimensional speckle-tracking echocardiography at baseline in 447 patients with HFpEF enrolled in the Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist (TOPCAT) trial. At a median follow-up of 2.6 years (interquartile range, 1.5-3.9 years), 115 patients experienced the primary composite outcome of cardiovascular death, HF hospitalization, or aborted cardiac arrest. Impaired LS, defined as an absolute LS <15.8%, was present in 52% of patients and was predictive of the composite outcome (adjusted hazard ratio, 2.14; 95% confidence interval, 1.26-3.66; P=0.005), cardiovascular death alone (adjusted hazard ratio, 3.20; 95% confidence interval, 1.44-7.12; P=0.004), and HF hospitalization alone (adjusted hazard ratio, 2.23; 95% confidence interval, 1.16-4.28; P=0.016) after adjustment for clinical and conventional echocardiographic variables. LS was the strongest echocardiographic predictor of the composite outcome. Exploratory analysis in a subset of 131 patients with follow-up LS assessed after 12 to 18 months demonstrated a trend toward improvement in LS associated with spironolactone in patients enrolled in the Americas but not in Russia or Georgia.
Conclusions: Impaired left ventricular systolic function is a powerful predictor of HF hospitalization, cardiovascular death, or aborted cardiac arrest in HFpEF independent of clinical predictors. Impaired LS represents a novel imaging biomarker to identify patients with HFpEF at particularly high risk for cardiovascular morbidity and mortality.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00094302.
Keywords: clinical trial; heart failure; heart ventricles; preserved left ventricular function; spironolactone; strain.
© 2015 American Heart Association, Inc.
Figures
Comment in
-
Longitudinal Strain in Heart Failure With Preserved Ejection Fraction: Is There a Role for Prognostication?Circulation. 2015 Aug 4;132(5):368-70. doi: 10.1161/CIRCULATIONAHA.115.017683. Epub 2015 Jun 30. Circulation. 2015. PMID: 26130120 No abstract available.
References
-
- Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, Gong Y, Liu P. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med. 2006;355:260–9. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–9. - PubMed
-
- Tsutsui H, Tsuchihashi M, Takeshita A. Mortality and readmission of hospitalized patients with congestive heart failure and preserved versus depressed systolic function. Am J Cardiol. 2001;88:530–3. - PubMed
-
- Smith GL, Masoudi FA, Vaccarino V, Radford MJ, Krumholz HM. Outcomes in heart failure patients with preserved ejection fraction: mortality, readmission, and functional decline. J Am Coll Cardiol. 2003;41:1510–8. - PubMed
-
- Vasan RS, Larson MG, Benjamin EJ, Evans JC, Reiss CK, Levy D. Congestive heart failure in subjects with normal versus reduced left ventricular ejection fraction: prevalence and mortality in a population-based cohort. J Am Coll Cardiol. 1999;33:1948–55. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- HHSN268200425207C/HC/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- K08 HL116792/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
