

A pharmacist-led follow-up program for patients with established coronary heart disease in North Norway - a randomized controlled trial
- PMID: 26131047
- PMCID: PMC4482847
- DOI: 10.18549/pharmpract.2015.02.575
A pharmacist-led follow-up program for patients with established coronary heart disease in North Norway - a randomized controlled trial
Abstract
Objectives: The aim of the study was twofold; 1) to develop a clinical pharmacist-led 12 month lasting follow-up program for patients with established coronary heart disease (CHD) discharged from the University Hospital of North Norway, and 2) to explore the impact of the program with regards to adherence to a medication assessment tool for secondary prevention of CHD and change in biomedical risk factors.
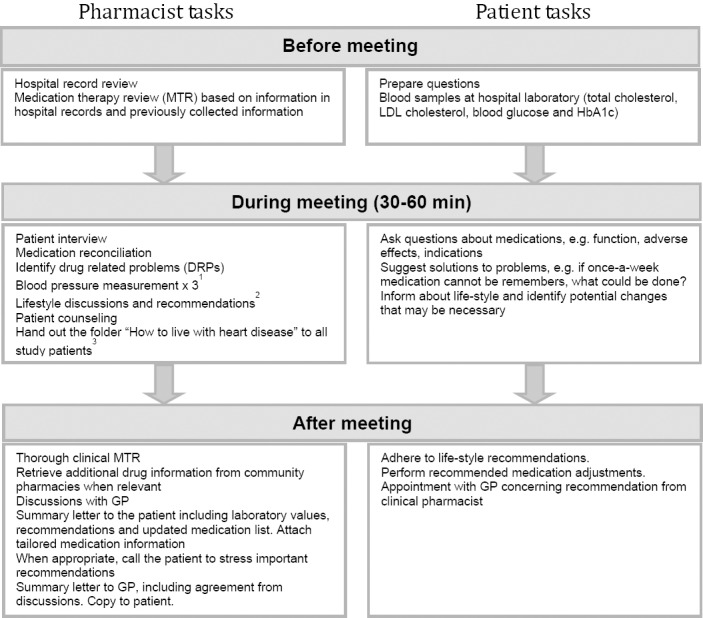
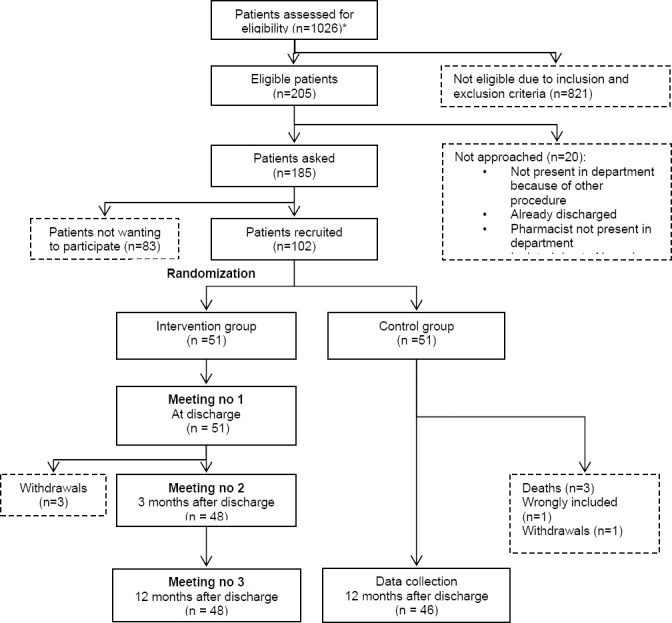
Methods: A total of 102 patients aged 18-82 years were enrolled in a non-blinded randomized controlled trial with an intervention group and a control group. The intervention comprised medication reconciliation, medication review and patient education during three meetings; at discharge, after three months and after twelve months. The control group received standard care from their general practitioner. Primary outcomes were adherence to clinical guideline recommendations concerning prescription, therapy goal achievement and lifestyle education defined in the medication assessment tool for secondary prevention of CHD (MAT-CHDSP). Secondary outcomes included changes in the biomedical risk factors cholesterol, blood pressure and blood glucose.
Results: Ninety-four patients completed the trial, 48 intervention group patients and 46 controls. Appropriate prescribing was high, but therapy goal achievement was low in both groups. Overall adherence to MAT-CHDSP criteria increased in both groups and was significantly higher in the intervention group at study end, 78.4% vs. 62.0%, p<0.001. The difference was statistically significant for the documented lifestyle advices in intervention group patients. No significant improvements in biomedical risk factors were observed in favor of the intervention group.
Conclusions: The study showed an increased guideline adherence in both study groups. This indicates that attention to clinical practice guideline recommendations in itself increases adherence - which may be a clinical pharmacist task. A larger adequately powered study is needed to show a significant difference in biomedical risk factor improvements in favor of the intervention. Amendments to the follow-up program are suggested before implementation in standard patient care can be recommended.
Keywords: Coronary Disease; Medication Reconciliation; Norway; Pharmaceutical Services; Pharmacists; Randomized Controlled Trials as Topic.
Conflict of interest statement
The authors declare that they have no conflicts of interest to disclose.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The laboratory expenses were covered by the Northern Norway Regional Health Authority.
Figures
- 1)
A calibrated GE Dinamap Pro 300 Patient Monitor and the correct sized cuff were utilized. A standardized three-time measurement procedure was where the average blood pressure was denoted and used for clinical evaluation.
- 2)
Discussion/information on diet and preparation of food, exercise advices. When patients wanted to stop smoking, they were much encouraged and were referred to the Norwegian’s authorities smoking cessation programs found at the webpage www.slutta.no or to the ’smoking telephone’ (a free phone-line where you meet professional personnel advising you on smoking cessation). When appropriate, the CP suggested choices of food and preparation of food and exercise. On request, or when needed, the CP printed lifestyle recommendations from the webpage of the Norwegian heart association and Norwegian diabetes association and handed out to patients (www.hjerte.no or www.diabetes.no)
- 3)
Published by the National Association for Heart and Lung Diseases (LHL). The folder includes information concerning heart disease, the most normal clinical procedures in relation to CHD, the most common drugs and lifestyle recommendations. Only handed out at the first meeting.
References
-
- Mackay J, Mensah G. Atlas of Heart Disease and Stroke. Geneve: WHO; 2004. ISBN:9789241562768.
-
- Causes of deaths. [accessed 2010 Jul 13];Statistisk sentralbyrå (Eng: Statistics Norway) 2010 Available from: URL: http://www.ssb.no .
-
- [accessed 2010 Jul 13];Scottish Intercollegate Guideline Network. Available from: URL: http://www.sign.ac.uk/
-
- National Institute of Health and Clinical Excellence. [accessed 2010 Jul 13]; Available from: URL: http://www.nice.org.uk/
-
- Nice Cardiovascular guidance. National Institute of Clinical Expertice (NICE) [accessed 2010 Jul 13];2011 Available from: URL: http://guidance.nice.org.uk/Topic/Cardiovascular .
LinkOut - more resources
Full Text Sources