

Rehospitalizations Following Sepsis: Common and Costly
- PMID: 26131597
- PMCID: PMC5044864
- DOI: 10.1097/CCM.0000000000001159
Rehospitalizations Following Sepsis: Common and Costly
Abstract
Objective: Although recent studies have shown that 30-day readmissions following sepsis are common, the overall fiscal impact of these rehospitalizations and their variability between hospitals relative to other high-risk conditions, such as congestive heart failure and acute myocardial infarction, are unknown. The objectives of this study were to characterize the frequency, cost, patient-level risk factors, and hospital-level variation in 30-day readmissions following sepsis compared with congestive heart failure and acute myocardial infarction.
Design: A retrospective cohort analysis of hospitalizations from 2009 to 2011.
Setting: All acute care, nonfederal hospitals in California.
Patients: Hospitalizations for sepsis (n = 240,198), congestive heart failure (n = 193,153), and acute myocardial infarction (n = 105,684) identified by administrative discharge codes.
Interventions: None.
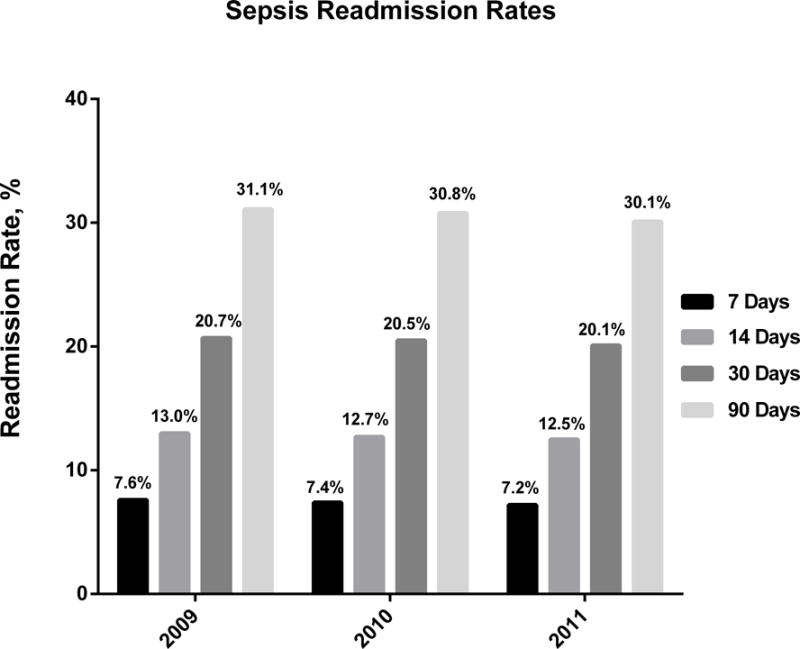
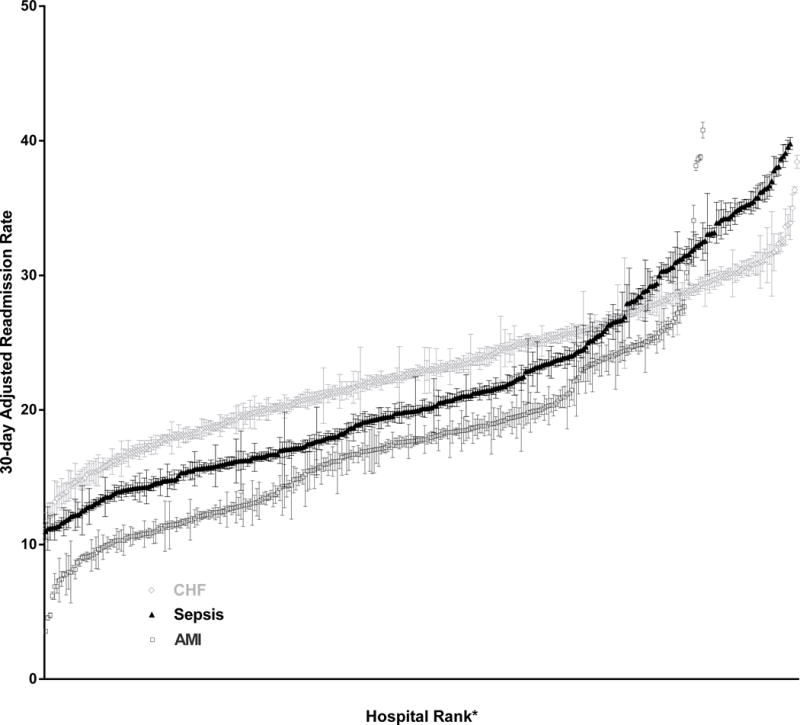
Measurements and main results: The primary outcomes were the frequency and cost of all-cause 30-day readmissions following hospitalization for sepsis compared with congestive heart failure and acute myocardial infarction. Variability in predicted readmission rates between hospitals was calculated using mixed-effects logistic regression analysis. The all-cause 30-day readmission rates were 20.4%, 23.6%, and 17.7% for sepsis, congestive heart failure, and acute myocardial infarction, respectively. The estimated annual costs of 30-day readmissions in the state of California during the study period were $500 million/yr for sepsis, $229 million/yr for congestive heart failure, and $142 million/yr for acute myocardial infarction. The risk- and reliability-adjusted readmission rates across hospitals ranged from 11.0% to 39.8% (median, 19.9%; interquartile range, 16.1-26.0%) for sepsis, 11.3% to 38.4% (median, 22.9%; interquartile range, 19.2-26.6%) for congestive heart failure, and 3.6% to 40.8% (median, 17.0%; interquartile range, 12.2-20.0%) for acute myocardial infarction. Patient-level factors associated with higher odds of 30-day readmission following sepsis included younger age, male gender, Black or Native American race, a higher burden of medical comorbidities, urban residence, and lower income.
Conclusion: Sepsis is a leading contributor to excess healthcare costs due to hospital readmissions. Interventions at clinical and policy levels should prioritize identifying effective strategies to reduce sepsis readmissions.
Conflict of interest statement
Disclosures: Drs. Chang, Tseng, and Shapiro have no conflicts of interest to declare.
Figures
Comment in
-
Sepsis Redux: Bigger and Badder Than Ever.Crit Care Med. 2015 Oct;43(10):2251-2. doi: 10.1097/CCM.0000000000001217. Crit Care Med. 2015. PMID: 26376250 No abstract available.
References
-
- Weissman JS, Ayanian JZ, Chasan-Taber S, Sherwood MJ, Roth C, Epstein AM. Hospital readmissions and quality of care. Medical care. 1999;37(5):490–501. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. The New England journal of medicine. 2009;360(14):1418–1428. - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Critical care medicine. 2001;29(7):1303–1310. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
