

Cutaneous Invasive Aspergillosis: Retrospective Multicenter Study of the French Invasive-Aspergillosis Registry and Literature Review
- PMID: 26131805
- PMCID: PMC4504535
- DOI: 10.1097/MD.0000000000001018
Cutaneous Invasive Aspergillosis: Retrospective Multicenter Study of the French Invasive-Aspergillosis Registry and Literature Review
Abstract
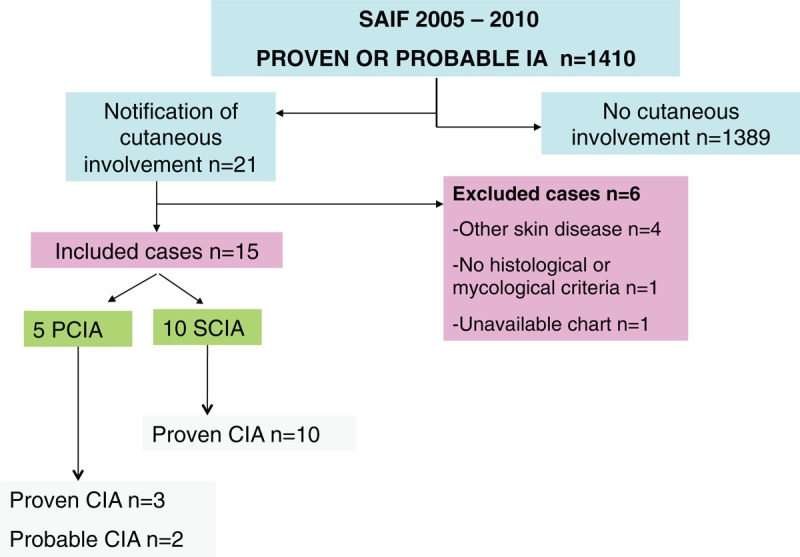
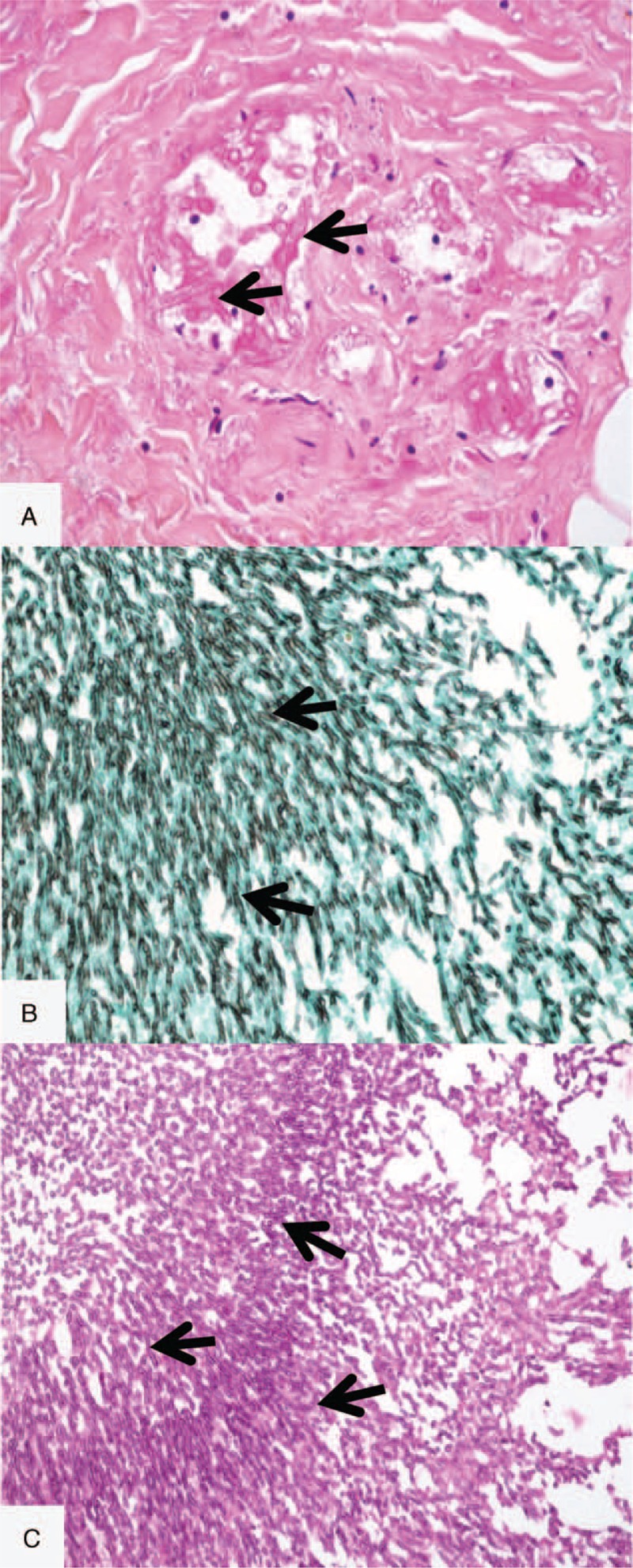
Invasive aspergillosis (IA) has poor prognosis in immunocompromised patients. Skin manifestations, when present, should contribute to an early diagnosis. The authors aimed to provide prevalence data and a clinical and histologic description of cutaneous manifestations of primary cutaneous IA (PCIA) and secondary CIA (SCIA) in a unique clinical series of IA and present the results of an exhaustive literature review of CIA. Cases of proven and probable IA with cutaneous manifestations were retrospectively extracted from those registered between 2005 and 2010 in a prospective multicenter aspergillosis database held by the National Reference Center for Invasive Mycoses and Antifungals, Pasteur Institute, France. Patients were classified as having PCIA (i.e., CIA without extracutaneous manifestations) or SCIA (i.e., disseminated IA). Among the 1,410 patients with proven or probable IA, 15 had CIA (1.06%), 5 PCIA, and 10 SCIA. Hematological malignancies were the main underlying condition (12/15). Patients with PCIA presented infiltrated and/or suppurative lesions of various localizations not related to a catheter site (4/5), whereas SCIA was mainly characterized by disseminated papules and nodules but sometimes isolated nodules or cellulitis. Histologic data were available for 11 patients, and for 9, similar for PCIA and SCIA, showed a dense dermal polymorphic inflammatory infiltrate, with the epidermis altered in PCIA only. Periodic acid Schiff and Gomori-Grocott methenamine silver nitrate staining for all but 2 biopsies revealed hyphae compatible with Aspergillus. Aspergillus flavus was isolated in all cases of PCIA, with Aspergillus fumigatus being the most frequent species (6/10) in SCIA. Two out 5 PCIA cases were treated surgically. The 3-month survival rate was 100% and 30% for PCIA and SCIA, respectively. Our study is the largest adult series of CIA and provides complete clinical and histologic data for the disease. Primary cutaneous IA should be recognized early, and cases of extensive necrosis should be treated surgically; its prognosis markedly differs from that for SCIA. Any suppurative, necrotic, papulonodular, or infiltrated skin lesion in an immunocompromised patient should lead to immediate biopsy for histologic analysis and mycological skin direct examination and culture.
Conflict of interest statement
Conflict of interest in link with the study: O.L. is consultant for Gilead Sciences, member of the speaker's bureau of Pfizer, MSD, Basilea, Astellas and Gilead Sciences. S.B. is consultant for Gilead Sciences, has received speaking honoraria from Pfizer and Gilead Sciences and travel grants from Astellas and Pfizer. K.S: no conflict.
Figures

Similar articles
-
Invasive aspergillosis in patients with acquired immunodeficiency syndrome: report of 33 cases. French Cooperative Study Group on Aspergillosis in AIDS.Am J Med. 1993 Aug;95(2):177-87. doi: 10.1016/0002-9343(93)90258-q. Am J Med. 1993. PMID: 8395142
-
Features of Invasive Aspergillosis Caused by Aspergillus flavus, France, 2012-2018.Emerg Infect Dis. 2025 May;31(5):896-905. doi: 10.3201/eid3105.241392. Emerg Infect Dis. 2025. PMID: 40305205 Free PMC article.
-
Clinical Features and Survival Outcomes of Invasive Aspergillosis in Pediatric Patients at a Medical School in Thailand.J Med Assoc Thai. 2016 Feb;99(2):150-8. J Med Assoc Thai. 2016. PMID: 27249894
-
Invasive aspergillosis in developing countries.Med Mycol. 2011 Apr;49 Suppl 1:S35-47. doi: 10.3109/13693786.2010.505206. Epub 2010 Aug 18. Med Mycol. 2011. PMID: 20718613 Review.
-
Primary aspergillosis affecting the tongue of a leukemic patient.Oral Dis. 2003 Jan;9(1):49-53. doi: 10.1034/j.1601-0825.2003.00883.x. Oral Dis. 2003. PMID: 12617259 Review.
Cited by
-
Diagnostic and therapeutic challenges of treating opportunistic fungal cellulitis: a case series.BMC Infect Dis. 2022 May 5;22(1):435. doi: 10.1186/s12879-022-07365-8. BMC Infect Dis. 2022. PMID: 35513796 Free PMC article.
-
Pediatric Invasive Aspergillosis.J Fungi (Basel). 2016 Jun 13;2(2):19. doi: 10.3390/jof2020019. J Fungi (Basel). 2016. PMID: 29376936 Free PMC article. Review.
-
Approach to the Solid Organ Transplant Patient with Suspected Fungal Infection.Infect Dis Clin North Am. 2016 Mar;30(1):277-96. doi: 10.1016/j.idc.2015.10.001. Epub 2015 Dec 28. Infect Dis Clin North Am. 2016. PMID: 26739603 Free PMC article. Review.
-
The Molecular Identification and Antifungal Susceptibility of Clinical Isolates of Aspergillus Section Flavi from Three French Hospitals.Microorganisms. 2023 Sep 28;11(10):2429. doi: 10.3390/microorganisms11102429. Microorganisms. 2023. PMID: 37894087 Free PMC article.
-
The skin and soft tissue infections in hematological patients.Curr Opin Infect Dis. 2020 Apr;33(2):101-109. doi: 10.1097/QCO.0000000000000632. Curr Opin Infect Dis. 2020. PMID: 32022740 Free PMC article. Review.
References
-
- De Pauw B, Walsh TJ, Donnelly JP, et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis 2008; 46:1813–1821. - PMC - PubMed
-
- Parody R, Martino R, Sánchez F, et al. Predicting survival in adults with invasive aspergillosis during therapy for hematological malignancies or after hematopoietic stem cell transplantation: single-center analysis and validation of the Seattle, French, and Strasbourg prognostic indexes. Am J Hematol 2009; 84:571–578. - PubMed
-
- McNeil MM, Nash SL, Hajjeh RA, et al. Trends in mortality due to invasive mycotic diseases in the United States, 1980–1997. Clin Infect Dis 2001; 33:641–647. - PubMed
-
- Lortholary O, Gangneux JP, Sitbon K, et al. French Mycosis Study Group. Epidemiological trends in invasive aspergillosis in France: the SAIF network (2005–2007). Clin Microbiol Infect 2011; 17:1882–1889. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
