

Percutaneous Aortic Balloon Valvuloplasty and Intracardiac Adrenaline in Electromechanical Dissociation as Bridge to Transcatheter Aortic Valve Implantation
- PMID: 26131825
- PMCID: PMC4504577
- DOI: 10.1097/MD.0000000000001061
Percutaneous Aortic Balloon Valvuloplasty and Intracardiac Adrenaline in Electromechanical Dissociation as Bridge to Transcatheter Aortic Valve Implantation
Abstract
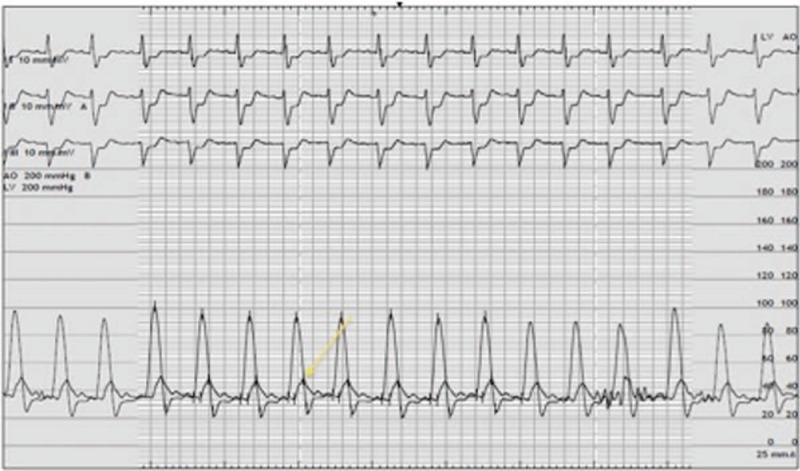
This report describes an emergent balloon aortic valvuloplasty (BAV) procedure performed under cardiopulmonary resuscitation in a 79-year-old man with severe symptomatic aortic stenosis (mean gradient 78 mm Hg, valve area 0.71 cm, and left ventricular ejection fraction 40%) awaiting surgery and who was admitted for heart failure rapidly evolving to cardiogenic shock and multiorgan failure. Decision was made to perform emergent BAV. After crossing the valve with a 6 French catheter, the patient developed an electromechanical dissociation confirmed at transesophageal echocardiography and cardiac arrest. Manual chest compressions were initiated along with the application of high doses of intravenous adrenaline, and BAV was performed under ongoing resuscitation. Despite BAV, transoesophageal echocardiography demonstrated no cardiac activity. At this point, it was decided to advance a pigtail catheter over the wire already in place in the left ventricle and to inject intracardiac adrenaline (1 mg, followed by 5 mg). Left ventricular contraction progressively resumed and, in the absence of aortic regurgitation, an intraaortic balloon pump was inserted. The patient could be weaned from intraaortic balloon pump and vasopressors on day 1, extubated on day 6, and recovered from multiorgan failure. In the absence of neurologic deficits, he underwent uneventful transcatheter aortic valve implantation on day 12 and was discharged to a cardiac rehabilitation program on day 30. At 3-month follow-up, he reported dyspnea NYHA class II as the only symptom.This case shows that severe aortic stenosis leading to electromechanical dissociation may be treated by emergent BAV and intracardiac administration of high-dose adrenaline. Intracardiac adrenaline may be considered in case of refractory electromechanical dissociation occurring in the cardiac catheterization laboratory.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures

References
-
- Cribier A, Savin T, Saoudi N, et al. Percutaneous transluminal valvuloplasty of acquired aortic stenosis in elderly patients: an alternative to valve replacement? Lancet 1986; 1:63–67. - PubMed
-
- Bashore TM, Berman AD, Davidson CJ, et al. Percutaneous balloon aortic valvuloplasty. Acute and 30-day follow-up results in 674 patients from the NHLBI Balloon Valvuloplasty Registry’. Circulation 1991; 84:2383–2397. - PubMed
-
- Otto CM, Mickel MC, Kennedy JW, et al. Three-year outcome after balloon aortic valvuloplasty. Insights into prognosis of valvular aortic stenosis. Circulation 1994; 89:642–650. - PubMed
-
- Davidson CJ, Harrison JK, Leithe ME, et al. Failure of balloon aortic valvuloplasty to result in sustained clinical improvement in patients with depressed left ventricular function. Am J Cardiol 1990; 65:72–77. - PubMed
-
- Shareghi S, Rasouli L, Shavelle DM, et al. Current results of balloon aortic valvuloplasty in high-risk patients. J Invasive Cardiol 2007; 19:1–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
