

Myocarditis in Patients With Antisynthetase Syndrome: Prevalence, Presentation, and Outcomes
- PMID: 26131832
- PMCID: PMC4504539
- DOI: 10.1097/MD.0000000000000798
Myocarditis in Patients With Antisynthetase Syndrome: Prevalence, Presentation, and Outcomes
Abstract
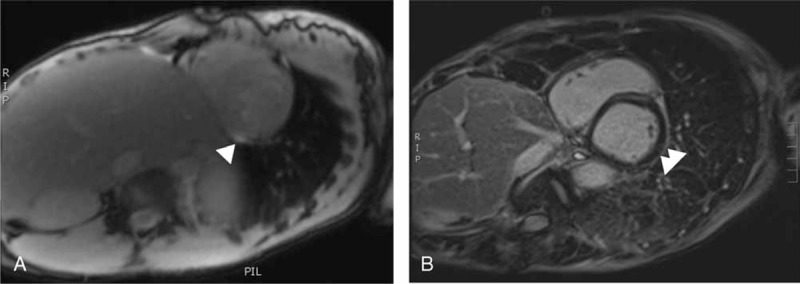
Antisynthetase syndrome (aSS) corresponds to an overlapping inflammatory myopathy identified by various myositis-specific autoantibodies (directed against tRNA-synthetases). Myocardial involvement in this condition is poorly described.From a registry of 352 aSS patients, 12 cases of myocarditis were retrospectively identified on the basis of an unexplained increase in troponin T/I levels associated with either suggestive cardiac magnetic resonance imaging (MRI) findings, nonsignificant coronary artery abnormalities or positive endomyocardial biopsy.The prevalence of myocarditis in aSS is 3.4% and was not linked to any autoantibody specificity: anti-Jo1 (n = 8), anti-PL7 (n = 3), and anti-PL12 (n = 1). Myocarditis was a part of the first aSS manifestations in 42% of the cases and was asymptomatic (n = 2) or revealed by an acute (n = 4) or a subacute (n = 6) cardiac failure. It should be noted that myocarditis was always associated with an active myositis. When performed (n = 11), cardiac MRI revealed a late hypersignal in the T1-images in 73% of the cases (n = 8). Half of the patients required intensive care. Ten patients (83%) received dedicated cardiotropic drugs. Steroids and at least 1 immunosuppressive drug were given in all cases. After a median follow-up of 11 months (range 0-84) 9 (75%) patients recovered whereas 3 (25%) developed a chronic cardiac insufficiency. No patient died.The prevalence of myocarditis in aSS is similar to that of other inflammatory myopathies. Although the prognosis is relatively good, myocarditis is a severe condition and should be carefully considered as a possible manifestation in active aSS patients.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Marguerie C, Bunn CC, Beynon HL, et al. Polymyositis, pulmonary fibrosis and autoantibodies to aminoacyl-tRNA synthetase enzymes. Q J Med 1990; 77:1019–1038. - PubMed
-
- Hervier B, Devilliers H, Stanciu R, et al. Hierarchical cluster and survival analyses of antisynthetase syndrome: phenotype and outcome are correlated with anti-tRNA synthetase antibody specificity. Autoimmun Rev 2012; 12:210–217. - PubMed
-
- Lundberg IE. The heart in dermatomyositis and polymyositis. Rheumatology 2006; 45:iv18–iv21. - PubMed
-
- Van Gelder H, Charles-Schoeman C. The heart in inflammatory myopathies. Rheum Dis Clin North Am 2014; 40:1–10. - PubMed
-
- Hervier B, Meyer A, Dieval C, et al. Pulmonary hypertension in antisynthetase syndrome: prevalence, aetiology and survival. Eur Respir J 2013; 42:1271–1282. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
