

Statin Effects on Aggression: Results from the UCSD Statin Study, a Randomized Control Trial
- PMID: 26132393
- PMCID: PMC4488854
- DOI: 10.1371/journal.pone.0124451
Statin Effects on Aggression: Results from the UCSD Statin Study, a Randomized Control Trial
Abstract
Background: Low/ered cholesterol is linked to aggression in some study designs. Cases/series have reported reproducible aggression increases on statins, but statins also bear mechanisms that could reduce aggression. Usual statin effects on aggression have not been characterized.
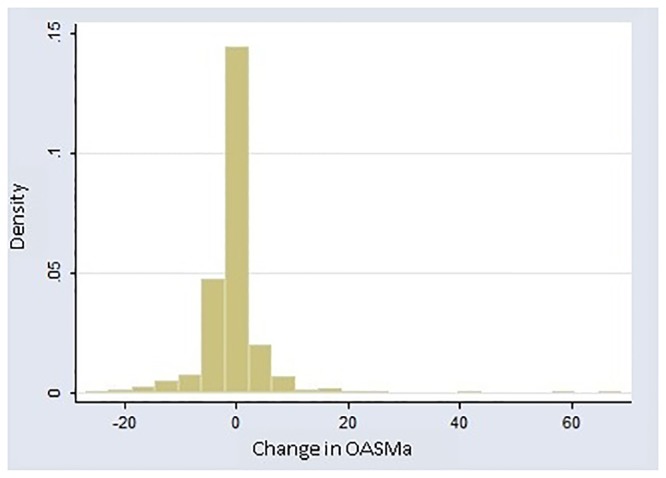
Methods: 1016 adults (692 men, 324 postmenopausal women) underwent double-blind sex-stratified randomization to placebo, simvastatin 20mg, or pravastatin 40mg (6 months). The Overt-Aggression-Scale-Modified-Aggression-Subscale (OASMa) assessed behavioral aggression. A significant sex-statin interaction was deemed to dictate sex-stratified analysis. Exploratory analyses assessed the influence of baseline-aggression, testosterone-change (men), sleep and age.
Results: The sex-statin interaction was significant (P=0.008). In men, statins tended to decrease aggression, significantly so on pravastatin: difference=-1.0(SE=0.49)P=0.038. Three marked outliers (OASMa-change ≥40 points) offset otherwise strong significance-vs-placebo: statins:-1.3(SE=0.38)P=0.0007; simvastatin:-1.4(SE=0.43)P=0.0011; pravastatin:-1.2(SE=0.45)P=0.0083. Age≤40 predicted greater aggression-decline on statins: difference=-1.4(SE=0.64)P=0.026. Aggression-protection was emphasized in those with low baseline aggression: age<40-and-low-baseline-aggression (N=40) statin-difference-vs-placebo=-2.4(SE=0.71)P=0.0016. Statins (especially simvastatin) lowered testosterone, and increased sleep problems. Testosterone-drop on statins predicted aggression-decline: β=0.64(SE=0.30)P=0.034, particularly on simvastatin: β=1.29(SE=0.49)P=0.009. Sleep-worsening on statins significantly predicted aggression-increase: β=2.2(SE=0.55)P<0.001, particularly on simvastatin (potentially explaining two of the outliers): β=3.3(SE=0.83)P<0.001. Among (postmenopausal) women, a borderline aggression-increase on statins became significant with exclusion of one younger, surgically-menopausal woman (N=310) β=0.70(SE=0.34)P=0.039. The increase was significant, without exclusions, for women of more typical postmenopausal age (≥45): (N=304) β=0.68(SE=0.34)P=0.048 - retaining significance with modified age-cutoffs (≥50 or ≥55). Significance was observed separately for simvastatin. The aggression-increase in women on statins was stronger in those with low baseline aggression (N=175) β=0.84(SE=0.30)P=0.006. No statin effect on whole blood serotonin was observed; and serotonin-change did not predict aggression-change.
Conclusion: Statin effects on aggression differed by sex and age: Statins generally decreased aggression in men; and generally increased aggression in women. Both findings were selectively prominent in participants with low baseline aggression - bearing lower change-variance, rendering an effect more readily evident.
Trial registration: Clinicaltrials.gov NCT00330980.
Conflict of interest statement
Figures

Similar articles
-
The UCSD Statin Study: a randomized controlled trial assessing the impact of statins on selected noncardiac outcomes.Control Clin Trials. 2004 Apr;25(2):178-202. doi: 10.1016/j.cct.2003.08.014. Control Clin Trials. 2004. PMID: 15020036 Free PMC article. Clinical Trial.
-
Reduction in blood pressure with statins: results from the UCSD Statin Study, a randomized trial.Arch Intern Med. 2008 Apr 14;168(7):721-7. doi: 10.1001/archinte.168.7.721. Arch Intern Med. 2008. PMID: 18413554 Free PMC article. Clinical Trial.
-
Consistency in efficacy and safety of ezetimibe coadministered with statins for treatment of hypercholesterolemia in women and men.J Womens Health (Larchmt). 2004 Dec;13(10):1101-7. doi: 10.1089/jwh.2004.13.1101. J Womens Health (Larchmt). 2004. PMID: 15650343
-
Conceptual foundations of the UCSD Statin Study: a randomized controlled trial assessing the impact of statins on cognition, behavior, and biochemistry.Arch Intern Med. 2004 Jan 26;164(2):153-62. doi: 10.1001/archinte.164.2.153. Arch Intern Med. 2004. PMID: 14744838 Free PMC article. Review.
-
Are statins created equal? Evidence from randomized trials of pravastatin, simvastatin, and atorvastatin for cardiovascular disease prevention.Am Heart J. 2006 Feb;151(2):273-81. doi: 10.1016/j.ahj.2005.04.003. Am Heart J. 2006. PMID: 16442888 Review.
Cited by
-
Effects of Statins and Cholesterol on Patient Aggression: Is There a Connection?Innov Clin Neurosci. 2018 Apr 1;15(3-4):24-27. Innov Clin Neurosci. 2018. PMID: 29707423 Free PMC article.
-
Formal comment on "Systematic review of the predictors of statin adherence for the primary prevention of cardiovascular disease".PLoS One. 2019 Jan 17;14(1):e0205138. doi: 10.1371/journal.pone.0205138. eCollection 2019. PLoS One. 2019. PMID: 30653537 Free PMC article.
-
Chocolate Consumption and Sex-Interest.Cureus. 2021 Feb 12;13(2):e13310. doi: 10.7759/cureus.13310. Cureus. 2021. PMID: 33643752 Free PMC article.
-
Post-Marketing Surveillance of Statins-A Descriptive Analysis of Psychiatric Adverse Reactions in EudraVigilance.Pharmaceuticals (Basel). 2022 Dec 10;15(12):1536. doi: 10.3390/ph15121536. Pharmaceuticals (Basel). 2022. PMID: 36558987 Free PMC article.
-
Mood, Personality, and Behavior Changes During Treatment with Statins: A Case Series.Drug Saf Case Rep. 2016 Dec;3(1):1. doi: 10.1007/s40800-015-0024-2. Drug Saf Case Rep. 2016. PMID: 27747681 Free PMC article.
References
-
- Golomb BA. Cholesterol and violence: Is there a connection? Annals of Internal Medicine. 1998;128:478–87. - PubMed
-
- Golomb BA, Stattin H, Mednick S. Low cholesterol and violent crime. J Psychiatr Res. 2000. Jul-Oct;34(4–5):301–9. . - PubMed
-
- Pekkanen J, Nissinen A, Punsar S, Karvonen M. Serum cholesterol and risk of accidental or violent death in a 25-year follow-up: the Finnish cohorts of the seven countries study. Arch Int Med. 1989;149:1589–91. - PubMed
-
- Neaton JD, Blackburn H, Jacobs D, Kuller L, Lee DJ, Sherwin R, et al. Serum cholesterol level and mortality findings for men screened in the Multiple Risk Factor Intervention Trial. Multiple Risk Factor Intervention Trial Research Group. Arch Intern Med. 1992. July;152(7):1490–500. . Epub 1992/07/01. eng. - PubMed
-
- Hillbrand M, Foster HG. Serum cholesterol levels and severity of aggression. Psychol Rep. 1993. February;72(1):270 . Epub 1993/02/01. eng. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
