

Lies, Damned Lies, and Health Inequality Measurements: Understanding the Value Judgments
- PMID: 26133019
- PMCID: PMC4521896
- DOI: 10.1097/EDE.0000000000000319
Lies, Damned Lies, and Health Inequality Measurements: Understanding the Value Judgments
Abstract
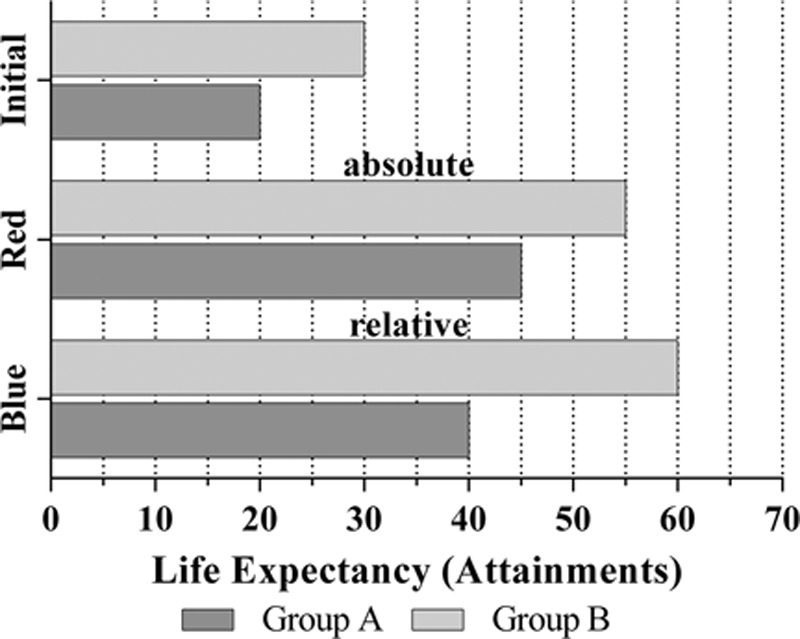
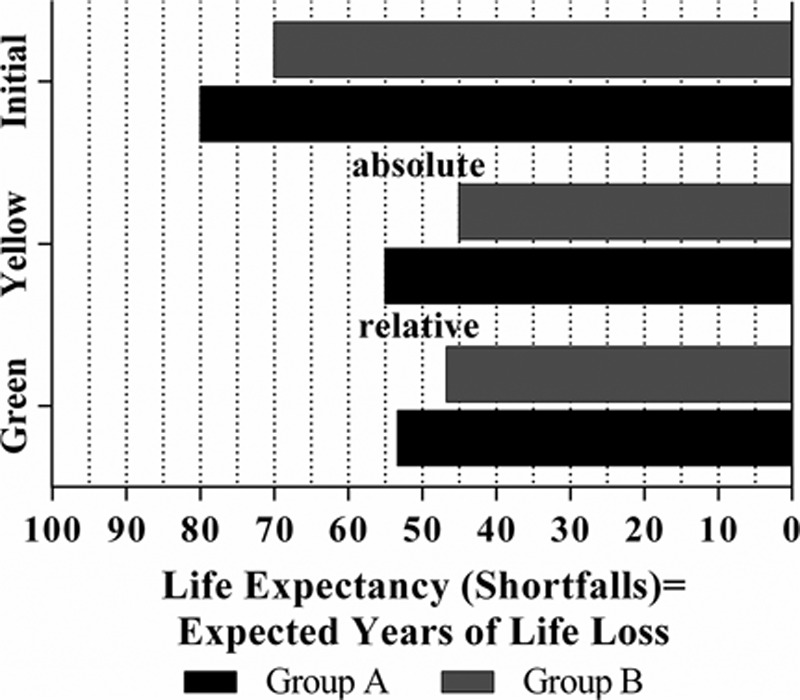
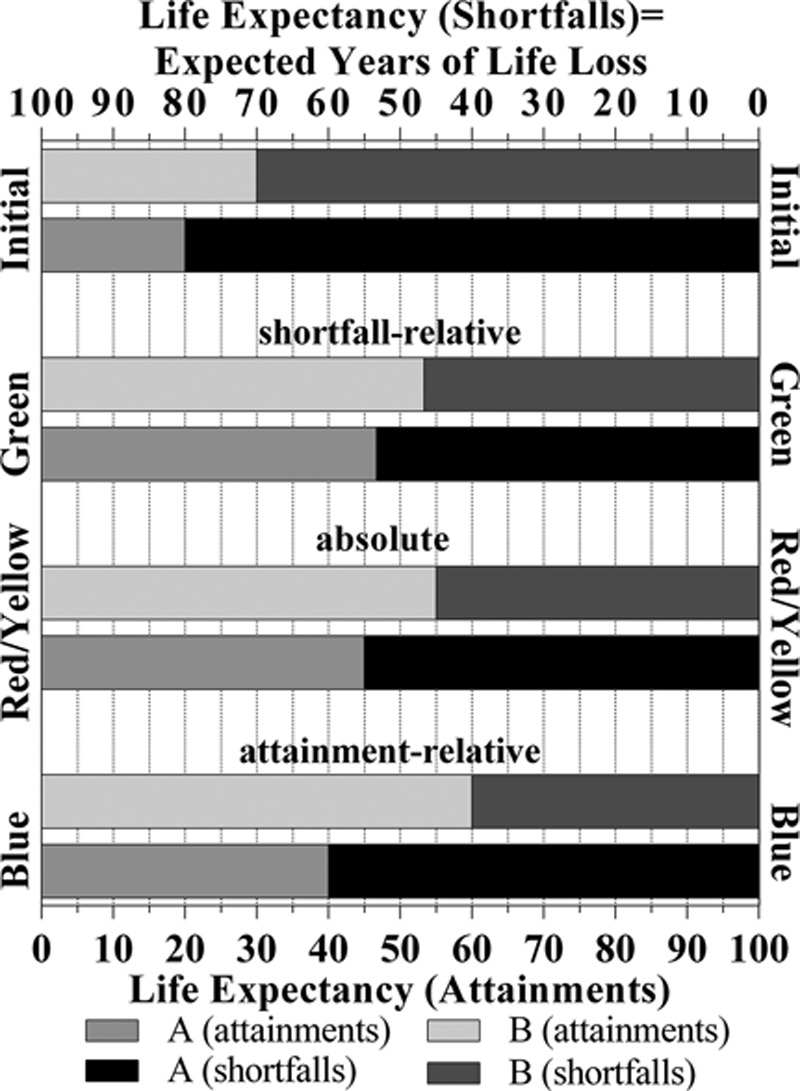
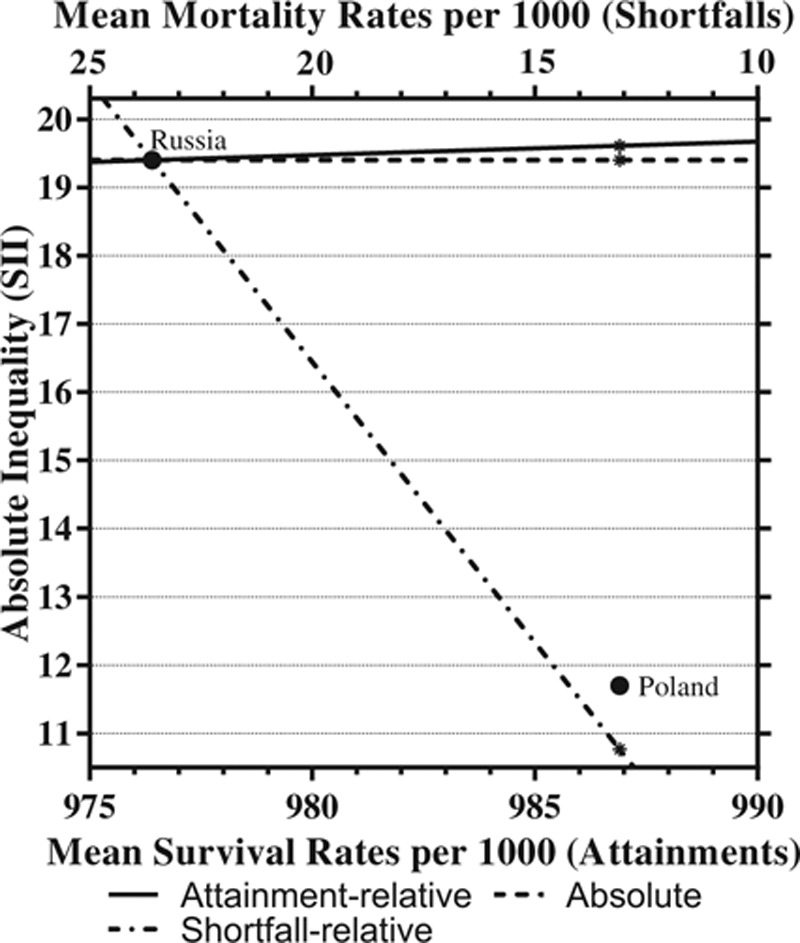
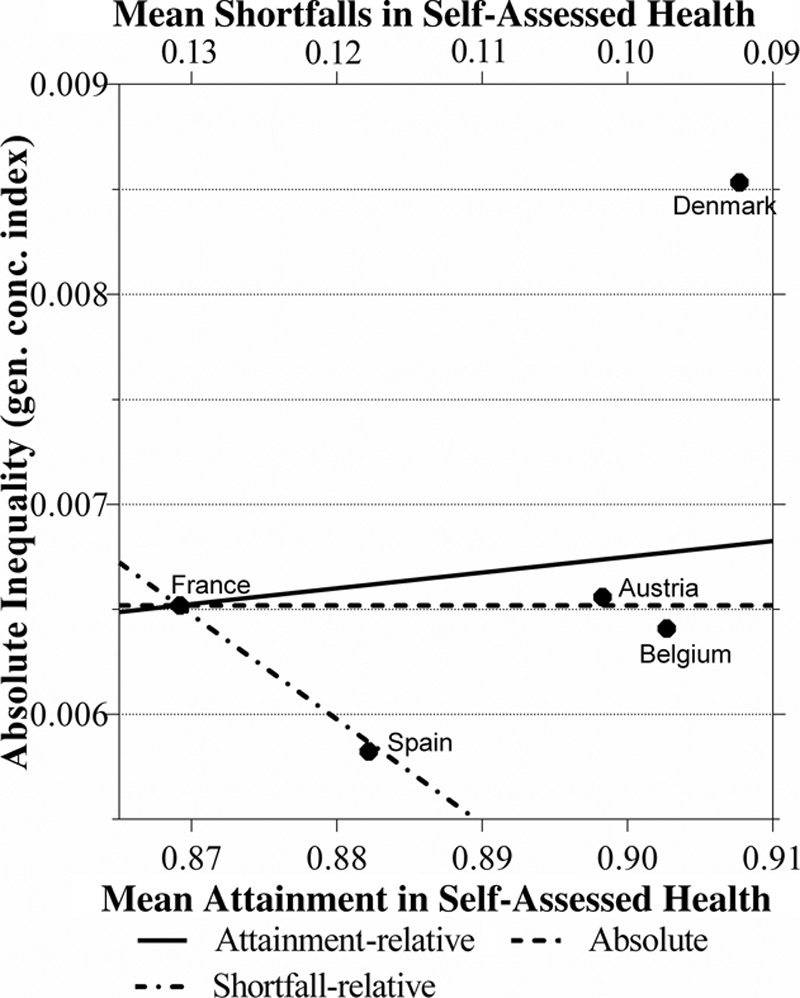
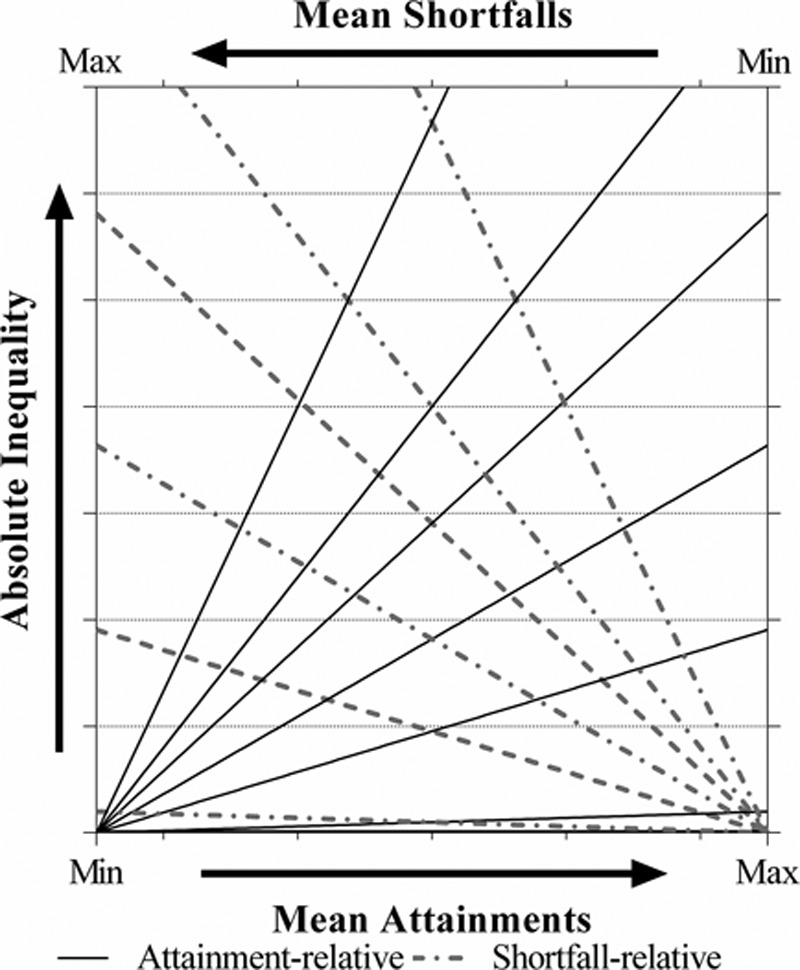
Measuring and monitoring socioeconomic health inequalities are critical for understanding the impact of policy decisions. However, the measurement of health inequality is far from value neutral, and one can easily present the measure that best supports one's chosen conclusion or selectively exclude measures. Improving people's understanding of the often implicit value judgments is therefore important to reduce the risk that researchers mislead or policymakers are misled. While the choice between relative and absolute inequality is already value laden, further complexities arise when, as is often the case, health variables have both a lower and upper bound, and thus can be expressed in terms of either attainments or shortfalls, such as for mortality/survival.We bring together the recent parallel discussions from epidemiology and health economics regarding health inequality measurement and provide a deeper understanding of the different value judgments within absolute and relative measures expressed both in attainments and shortfalls, by graphically illustrating both hypothetical and real examples. We show that relative measures in terms of attainments and shortfalls have distinct value judgments, highlighting that for health variables with two bounds the choice is no longer only between an absolute and a relative measure but between an absolute, an attainment- relative and a shortfall-relative one. We illustrate how these three value judgments can be combined onto a single graph which shows the rankings according to all three measures, and illustrates how the three measures provide ethical benchmarks against which to judge the difference in inequality between populations.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Comment in
-
Commentary: Value Judgments in Health Inequality Measurement.Epidemiology. 2015 Sep;26(5):670-2. doi: 10.1097/EDE.0000000000000357. Epidemiology. 2015. PMID: 26133020 Free PMC article. No abstract available.
-
Re: Lies, Damned Lies, and Health Inequality Measurements: Understanding the Value Judgments.Epidemiology. 2016 May;27(3):e15-6. doi: 10.1097/EDE.0000000000000440. Epidemiology. 2016. PMID: 26808600 Free PMC article. No abstract available.
-
The Authors Respond.Epidemiology. 2016 May;27(3):e16-7. doi: 10.1097/EDE.0000000000000441. Epidemiology. 2016. PMID: 26808602 No abstract available.
-
Trends in Relative Inequalities in Measures of Favorable and Adverse Population Health Outcomes.Epidemiology. 2017 May;28(3):e23-e24. doi: 10.1097/EDE.0000000000000625. Epidemiology. 2017. PMID: 28151745 No abstract available.
References
-
- Mackenbach JP, Stirbu I, Roskam AJ, et al. European Union Working Group on Socioeconomic Inequalities in Health. Socioeconomic inequalities in health in 22 European countries. N Engl J Med. 2008;358:2468–2481. - PubMed
-
- van Doorslaer E, Koolman X. Explaining the differences in income-related health inequalities across European countries. Health Econ. 2004;13:609–628. - PubMed
-
- Wagstaff A. Inequality aversion, health inequalities and health achievement. J Health Econ. 2002;21:627–641. - PubMed
-
- Harper S, Lynch J. Measuring health inequalities. Methods Soc Epidemiol. 2006;1:134.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
