

Misclassification of Breast Imaging Reporting and Data System (BI-RADS) Mammographic Density and Implications for Breast Density Reporting Legislation
- PMID: 26133090
- PMCID: PMC4558212
- DOI: 10.1111/tbj.12443
Misclassification of Breast Imaging Reporting and Data System (BI-RADS) Mammographic Density and Implications for Breast Density Reporting Legislation
Abstract
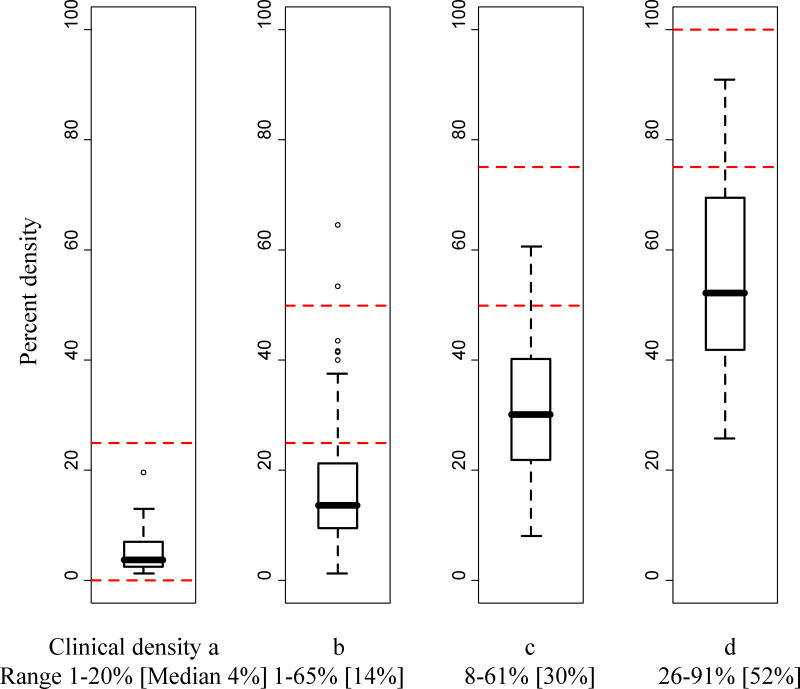
USA states have begun legislating mammographic breast density reporting to women, requiring that women undergoing screening mammography who have dense breast tissue (Breast Imaging Reporting and Data System [BI-RADS] density c or d) receive written notification of their breast density; however, the impact that misclassification of breast density will have on this reporting remains unclear. The aim of this study was to assess reproducibility of the four-category BI-RADS density measure and examine its relationship with a continuous measure of percent density. We enrolled 19 radiologists, experienced in breast imaging, from a single integrated health care system. Radiologists interpreted 341 screening mammograms at two points in time 6 months apart. We assessed intra- and interobserver agreement in radiologists'; interpretations of BI-RADS density and explored whether agreement depended upon radiologist characteristics. We examined the relationship between BI-RADS density and percent density in a subset of 282 examinations. Intraradiologist agreement was moderate to substantial, with kappa varying across radiologists from 0.50 to 0.81 (mean = 0.69, 95% CI [0.63, 0.73]). Intraradiologist agreement was higher for radiologists with ≥10 years experience interpreting mammograms (difference in mean kappa = 0.10, 95% CI [0.01, 0.24]). Interradiologist agreement varied widely across radiologist pairs from slight to substantial, with kappa ranging from 0.02 to 0.72 (mean = 0.46, 95% CI [0.36, 0.55]). Of 145 examinations interpreted as "nondense" (BI-RADS density a or b) by the majority of radiologists, 82.8% were interpreted as "dense" (BI-RADS density c or d) by at least one radiologist. Of 187 examinations interpreted as "dense" by the majority of radiologists, 47.1% were interpreted as "nondense" by at least one radiologist. While the examinations of almost half of the women in our study were interpreted clinically as having BI-RADS density c or d, only about 10% of examinations had percent density >50%. Our results suggest that breast density reporting based on a single BI-RADS density interpretation may be misleading due to high interradiologist variability and a lack of correspondence between BI-RADS density and percent density.
Keywords: BI-RADS density; breast density reporting legislation; intra- and interradiologist agreement; misclassification; percent density.
© 2015 Wiley Periodicals, Inc.
Figures


Similar articles
-
Inter- and intraradiologist variability in the BI-RADS assessment and breast density categories for screening mammograms.Br J Radiol. 2012 Nov;85(1019):1465-70. doi: 10.1259/bjr/21256379. Epub 2012 Sep 19. Br J Radiol. 2012. PMID: 22993385 Free PMC article.
-
Assessment of Interradiologist Agreement Regarding Mammographic Breast Density Classification Using the Fifth Edition of the BI-RADS Atlas.AJR Am J Roentgenol. 2016 May;206(5):1119-23. doi: 10.2214/AJR.15.15049. Epub 2016 Mar 21. AJR Am J Roentgenol. 2016. PMID: 26999655
-
Measuring mammographic density: comparing a fully automated volumetric assessment versus European radiologists' qualitative classification.Eur Radiol. 2016 Dec;26(12):4354-4360. doi: 10.1007/s00330-016-4309-3. Epub 2016 Mar 24. Eur Radiol. 2016. PMID: 27011371 Free PMC article. Clinical Trial.
-
Predictors of interobserver agreement in breast imaging using the Breast Imaging Reporting and Data System.Breast Cancer Res Treat. 2010 Apr;120(3):539-46. doi: 10.1007/s10549-010-0770-x. Epub 2010 Feb 21. Breast Cancer Res Treat. 2010. PMID: 20300960 Free PMC article. Review.
-
Micronucleus Test for Diagnosing Uncertain Cases (BI-RADS 3) in Breast Cancer Screening: A Review and Preliminary Results.Gulf J Oncolog. 2020 Jan;1(32):45-50. Gulf J Oncolog. 2020. PMID: 32342918 Review.
Cited by
-
Comparison of breast density assessments according to BI-RADS 4th and 5th editions and experience level.Acta Radiol Open. 2020 Jul 20;9(7):2058460120937381. doi: 10.1177/2058460120937381. eCollection 2020 Jul. Acta Radiol Open. 2020. PMID: 32733694 Free PMC article.
-
Investigating the added value of incorporatingmammographic density to an integrated breastcancer risk model with questionnaire-based riskfactors and polygenic risk score.Res Sq [Preprint]. 2024 Dec 19:rs.3.rs-5445786. doi: 10.21203/rs.3.rs-5445786/v1. Res Sq. 2024. PMID: 39764121 Free PMC article. Preprint.
-
The effect of volumetric breast density on the risk of screen-detected and interval breast cancers: a cohort study.Breast Cancer Res. 2017 Jun 5;19(1):67. doi: 10.1186/s13058-017-0859-9. Breast Cancer Res. 2017. PMID: 28583146 Free PMC article.
-
Summary measures of agreement and association between many raters' ordinal classifications.Ann Epidemiol. 2017 Oct;27(10):677-685.e4. doi: 10.1016/j.annepidem.2017.09.001. Epub 2017 Sep 22. Ann Epidemiol. 2017. PMID: 29029991 Free PMC article. Review.
-
Volumetric breast density and risk of advanced cancers after a negative screening episode: a cohort study.Breast Cancer Res. 2018 Aug 9;20(1):95. doi: 10.1186/s13058-018-1025-8. Breast Cancer Res. 2018. PMID: 30092817 Free PMC article.
References
-
- McCormack VA, dos Santos Silva I. Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidem Biomar. 2006;15(6):1159–69. - PubMed
-
- Carney PA, Miglioretti DL, Yankaskas BC, et al. Individual and combined effects of age, breast density, and hormone replacement therapy use on the accuracy of screening mammography. Ann Intern Med. 2003;138(3):168–75. - PubMed
-
- Kerlikowske K, Grady D, Barclay J, Sickles EA, Ernster V. Effect of age, breast density, and family history on the sensitivity of first screening mammography. J Amer Med Assoc. 1996;276(1):33–8. - PubMed
-
- Buist DSM, Porter PL, Lehman C, Taplin SH, White E. Factors contributing to mammography failure in women aged 40–49 years. J Natl Cancer I. 2004;96(19):1432–40. - PubMed
-
- American College of Radiology. Breast Imaging Reporting and Data System. 5. Reston, VA: American College of Radiology; 2013.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
