

A Cost-Effectiveness Analysis of First Trimester Non-Invasive Prenatal Screening for Fetal Trisomies in the United States
- PMID: 26133556
- PMCID: PMC4489811
- DOI: 10.1371/journal.pone.0131402
A Cost-Effectiveness Analysis of First Trimester Non-Invasive Prenatal Screening for Fetal Trisomies in the United States
Abstract
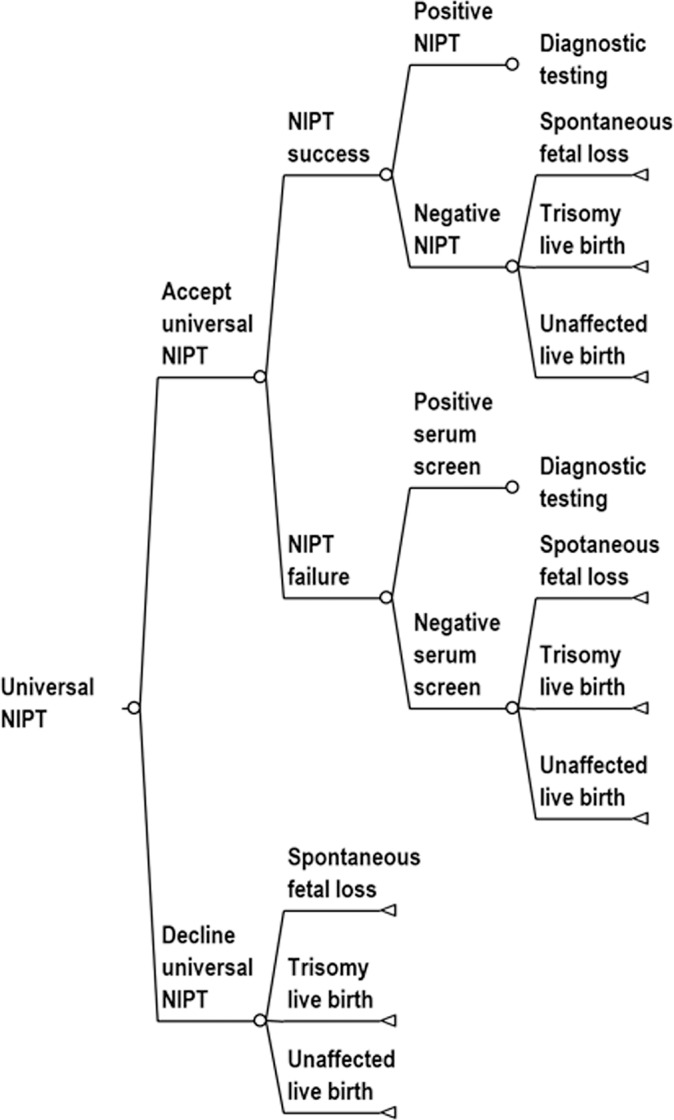
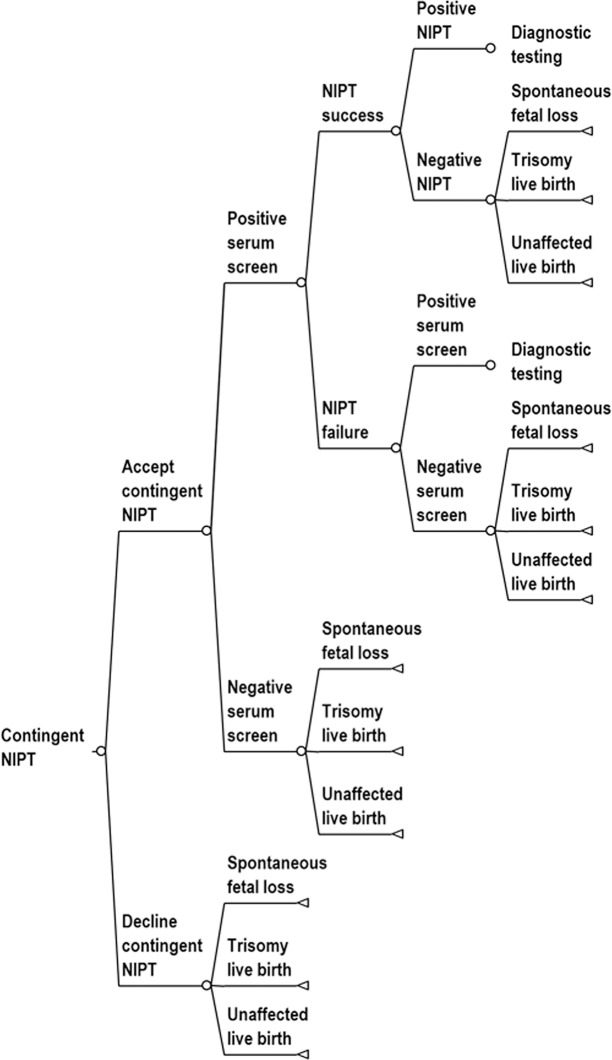
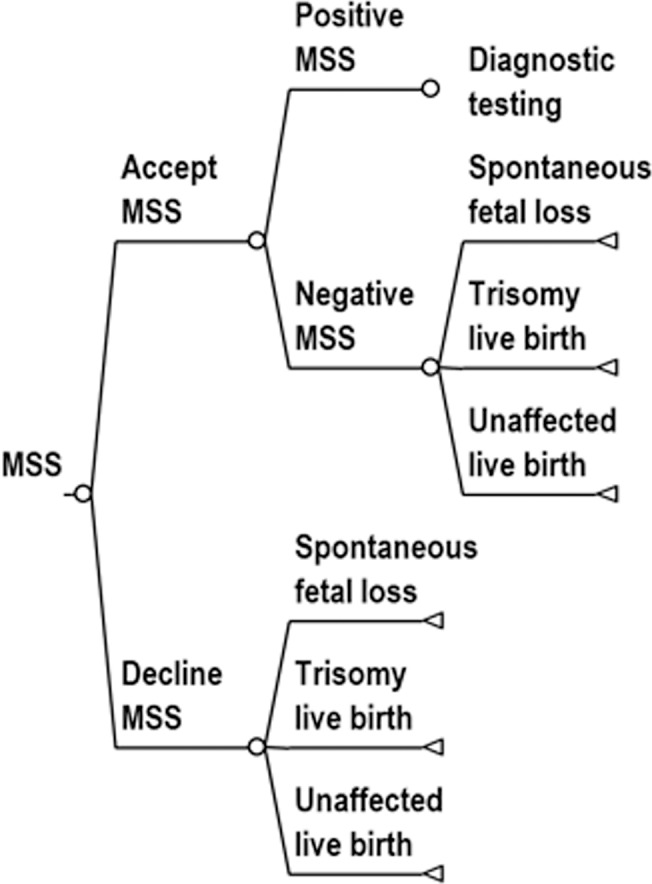
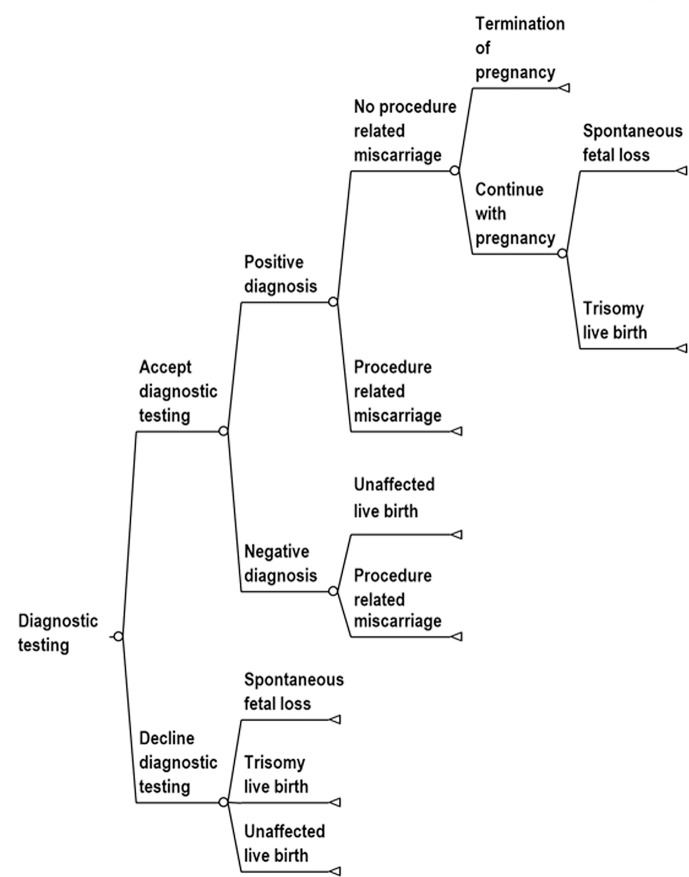
Background: Non-invasive prenatal testing (NIPT) is a relatively new technology for diagnosis of fetal aneuploidies. NIPT is more accurate than conventional maternal serum screening (MSS) but is also more costly. Contingent NIPT may provide a cost-effective alternative to universal NIPT screening. Contingent screening used a two-stage process in which risk is assessed by MSS in the first stage and, based on a risk cutoff, high-risk pregnancies are referred for NIPT. The objective of this study was to (1) determine the optimum MSS risk cutoff for contingent NIPT and (2) compare the cost effectiveness of optimized contingent NIPT to universal NIPT and conventional MSS.
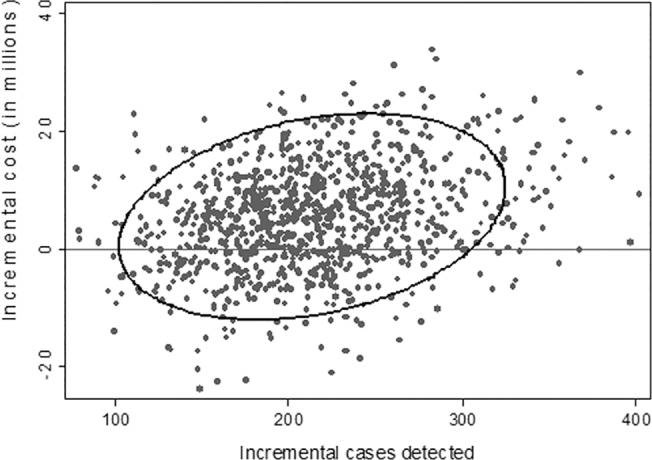
Study design: Decision-analytic model using micro-simulation and probabilistic sensitivity analysis. We evaluated cost effectiveness from three perspectives: societal, governmental, and payer.
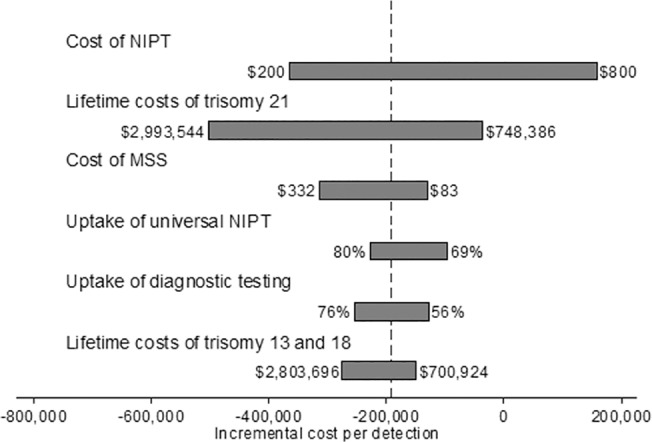
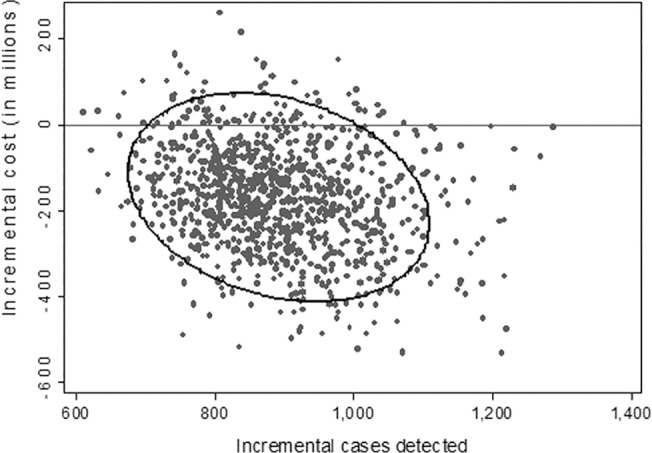
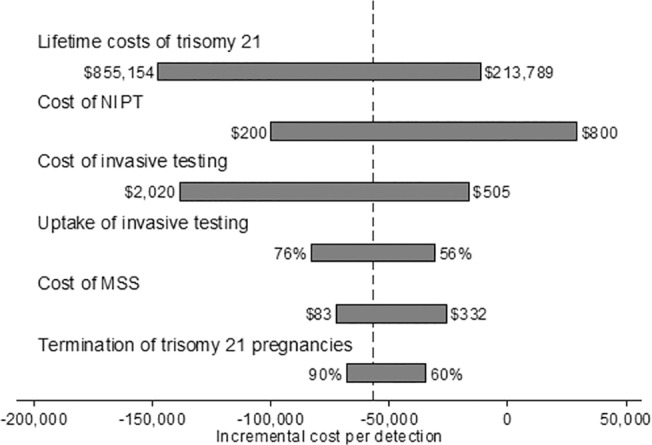
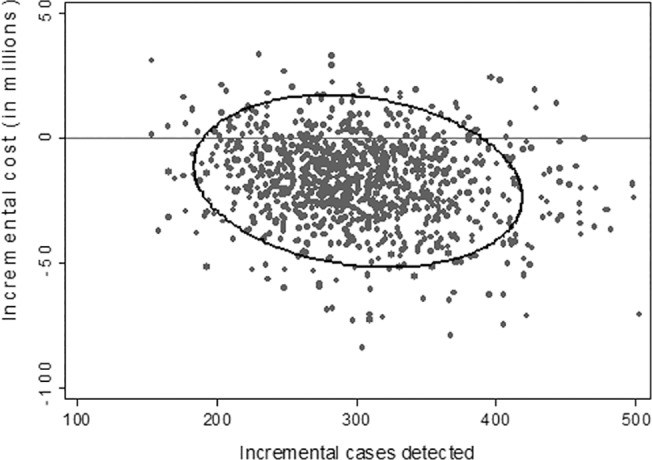
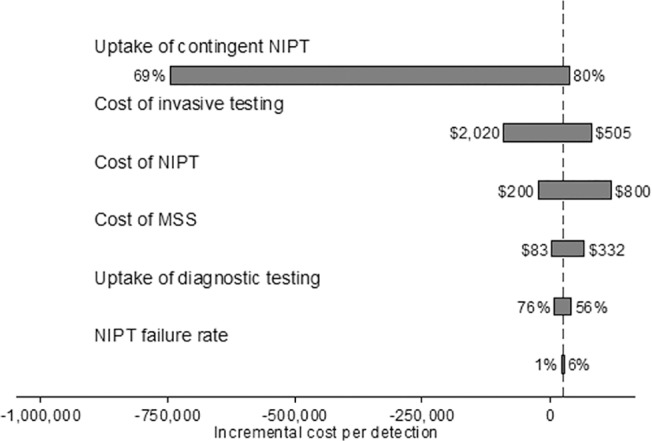
Results: From a societal perspective, universal NIPT dominated both contingent NIPT and MSS. From a government and payer perspective, contingent NIPT dominated MSS. Compared to contingent NIPT, adopting a universal NIPT would cost $203,088 for each additional case detected from a government perspective and $263,922 for each additional case detected from a payer perspective.
Conclusions: From a societal perspective, universal NIPT is a cost-effective alternative to MSS and contingent NIPT. When viewed from narrower perspectives, contingent NIPT is less costly than universal NIPT and provides a cost-effective alternative to MSS.
Conflict of interest statement
Figures
References
-
- Gil MM, Akolekar R, Quezada MS, Bregant B, Nicolaides KH (2014) Analysis of cell-free DNA in maternal blood in screening for aneuploidies: meta-analysis. Fetal Diagn Ther 35: 156–173. - PubMed
-
- Non-Invasive Prenatal Testing (NIPT). this is my: Health Screening & Ultrasound Centres.
-
- Walker BS, Jackson BR, LaGrave D, Ashwood ER, Schmidt RL (2014) A cost-effectiveness analysis of cell free DNA as a replacement for serum screening for Down syndrome. Prenat Diagn. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
