

A conceptual framework: the early and late phases of skeletal muscle dysfunction in the acute respiratory distress syndrome
- PMID: 26134116
- PMCID: PMC4488983
- DOI: 10.1186/s13054-015-0979-5
A conceptual framework: the early and late phases of skeletal muscle dysfunction in the acute respiratory distress syndrome
Abstract
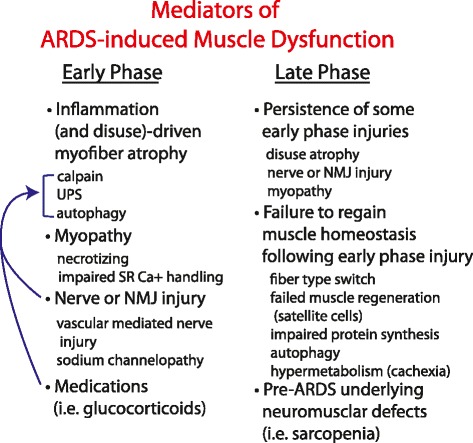
Patients with acute respiratory distress syndrome (ARDS) often develop severe diaphragmatic and limb skeletal muscle dysfunction. Impaired muscle function in ARDS is associated with increased mortality, increased duration of mechanical ventilation, and functional disability in survivors. In this review, we propose that muscle dysfunction in ARDS can be categorized into an early and a late phase. These early and late phases are based on the timing in relationship to lung injury and the underlying mechanisms. The early phase occurs temporally with the onset of lung injury, is driven by inflammation and disuse, and is marked predominantly by muscle atrophy from increased protein degradation. The ubiquitin-proteasome, autophagy, and calpain-caspase pathways have all been implicated in early-phase muscle dysfunction. Late-phase muscle weakness persists in many patients despite resolution of lung injury and cessation of ongoing acute inflammation-driven muscle atrophy. The clinical characteristics and mechanisms underlying late-phase muscle dysfunction do not involve the massive protein degradation and atrophy of the early phase and may reflect a failure of the musculoskeletal system to regain homeostatic balance. Owing to these underlying mechanistic differences, therapeutic interventions for treating muscle dysfunction in ARDS may differ during the early and late phases. Here, we review clinical and translational investigations of muscle dysfunction in ARDS, placing them in the conceptual framework of the early and late phases. We hypothesize that this conceptual model will aid in the design of future mechanistic and clinical investigations of the skeletal muscle system in ARDS and other critical illnesses.
Figures

References
-
- Rubenfeld GD, Caldwell E, Peabody E, Weaver J, Martin DP, Neff M, et al. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353:1685–93. - PubMed
-
- Brinkman S, Bakhshi-Raiez F, Abu-Hanna A, de Jonge E, de Keizer NF. Determinants of mortality after hospital discharge in ICU patients: literature review and Dutch cohort study. Crit Care Med. 2013;41:1237–51. - PubMed
-
- Lone NI, Walsh TS. Impact of intensive care unit organ failures on mortality during the five years after a critical illness. Am J Respir Crit Care Med. 2012;186:640–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
